Preparing your business tax certificate form can be a daunting task, especially if it's your first time filing taxes. Not only do you need to know what to include in the form, but also how and when to submit it. But don't worry! Our blog post will provide all of the information you need about completing this important document for businesses in accordance with state law requirements. We'll cover topics such as what is required on the form itself, any special instructions needed for filing correctly and on time, as well as common mistakes that should be avoided when filling out forms. Follow along with us today and get ready to become an expert at submitting your business tax certficate form!
| Question | Answer |
|---|---|
| Form Name | Pay Business Tax Certificate Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Business Tax Certificate Application - City of Inglewood |
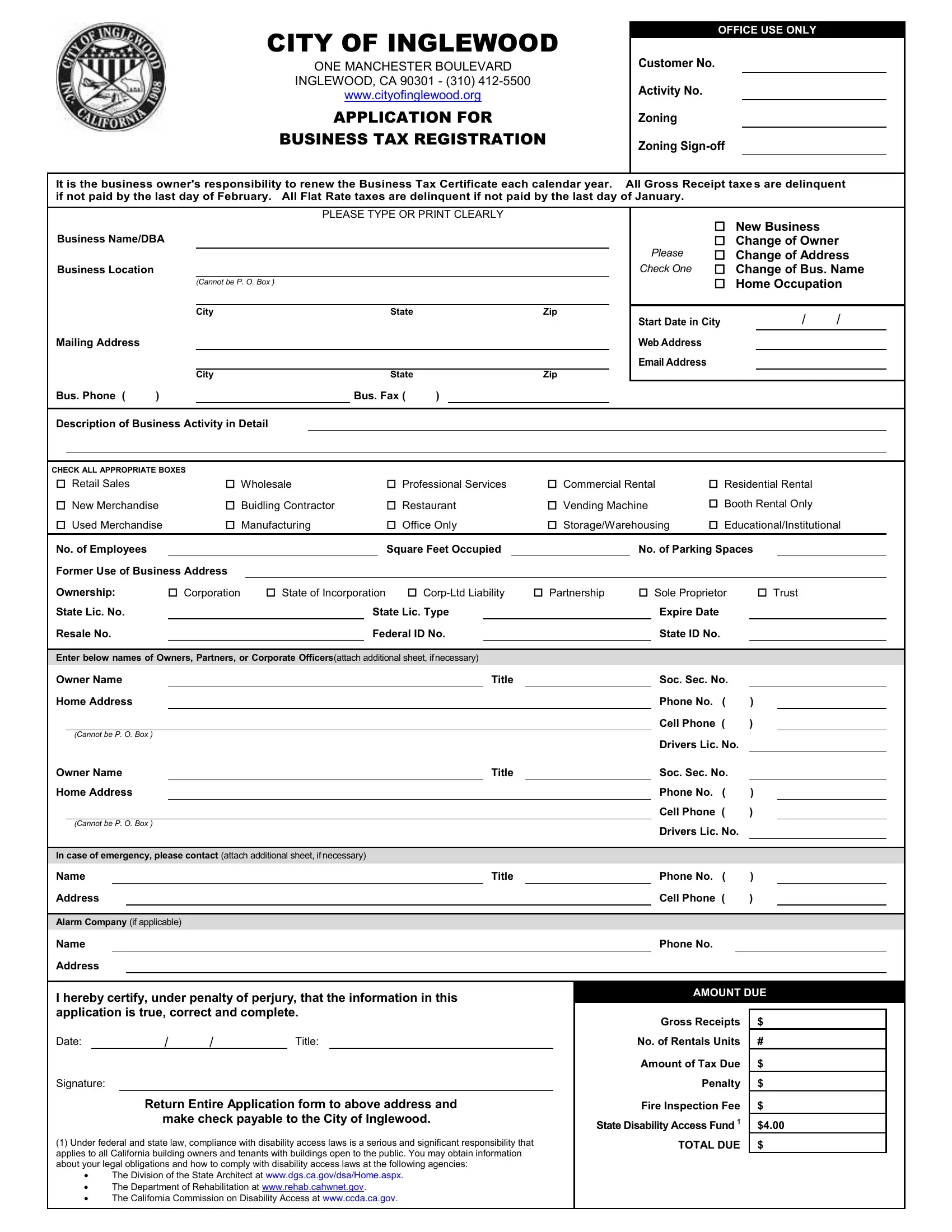
CITY OF INGLEWOOD
ONE MANCHESTER BOULEVARD
INGLEWOOD, CA 90301 - (310)
www.cityofinglewood.org
APPLICATION FOR
BUSINESS TAX REGISTRATION
OFFICE USE ONLY
Customer No.
Activity No.
Zoning
Zoning
It is the business owner's responsibility to renew the Business Tax Certificate each calendar year. All Gross Receipt taxes are delinquent if not paid by the last day of February. All Flat Rate taxes are delinquent if not paid by the last day of January.
|
|
|
PLEASE TYPE OR PRINT CLEARLY |
|||
Business Name/DBA |
|
|
|
|
||
Business Location |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(CANNOT BE P. O. BOX ) |
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
State |
|
Zip |
Mailing Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
State |
|
Zip |
Bus. Phone ( |
) |
|
|
Bus. Fax ( |
) |
|
|
New Business |
|
Change of Owner |
PLEASE |
Change of Address |
CHECK ONE |
Change of Bus. Name |
|
Home Occupation |
Start Date in City |
/ |
/ |
Web Address |
|
|
Email Address |
|
|
Description of Business Activity in Detail
CHECK ALL APPROPRIATE BOXES |
|
|
|
|
Retail Sales |
Wholesale |
Professional Services |
Commercial Rental |
Residential Rental |
New Merchandise |
Buidling Contractor |
Restaurant |
Vending Machine |
Booth Rental Only |
Used Merchandise |
Manufacturing |
Office Only |
Storage/Warehousing |
Educational/Institutional |
|
No. of Employees |
|
|
|
|
|
|
|
Square Feet Occupied |
|
|
|
|
|
No. of Parking Spaces |
|
|
||||||||||
|
Former Use of Business Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Ownership: |
|
Corporation |
State of Incorporation |
|
Partnership |
Sole Proprietor |
Trust |
|
||||||||||||||||||
|
State Lic. No. |
|
|
|
|
|
|
State Lic. Type |
|
|
|
|
|
|
Expire Date |
|
|
|
|||||||||
|
Resale No. |
|
|
|
|
|
|
|
|
|
Federal ID No. |
|
|
|
|
|
|
State ID No. |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Enter below names of Owners, Partners, or Corporate Officers(attach additional sheet, ifnecessary) |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
Owner Name |
|
|
|
|
|
|
|
|
|
Title |
|
|
|
|
|
Soc. Sec. No. |
|
|
|
|||||||
|
Home Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone No. ( |
) |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cell Phone ( |
) |
|
|
|
|
|
(CANNOT BE P. O. BOX ) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Drivers Lic. No. |
|
|
|
|
|
Owner Name |
|
|
|
|
|
|
|
|
|
Title |
|
|
|
|
|
Soc. Sec. No. |
|
|
|
|||||||
|
Home Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone No. ( |
) |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cell Phone ( |
) |
|
|
|
|
|
(CANNOT BE P. O. BOX ) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Drivers Lic. No. |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
In case of emergency, please contact (attach additional sheet, ifnecessary) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
Title |
|
|
|
|
|
Phone No. ( |
) |
|
|
||||
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cell Phone ( |
) |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Alarm Company (if applicable) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone No. |
|
|
|
|||
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
I hereby certify, under penalty of perjury, that the information in this |
|
|
|
|
|
AMOUNT DUE |
|
|||||||||||||||||||
|
application is true, correct and complete. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
Gross Receipts |
$ |
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Date: |
|
|
|
/ |
/ |
|
Title: |
|
|
|
|
|
|
|
No. of Rentals Units |
# |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Amount of Tax Due |
$ |
|
|
||
|
Signature: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Penalty |
$ |
|
|
|||
|
|
|
|
|
|
Return Entire Application form to above address and |
|
|
|
|
Fire Inspection Fee |
$ |
|
|
|||||||||||||
|
|
|
|
|
|
|
make check payable to the City of Inglewood. |
|
|
|
State Disability Access Fund 1 |
$4.00 |
|
||||||||||||||
|
(1) Under federal and state law, compliance with disability access laws is a serious and significant responsibility that |
|
|
|
TOTAL DUE |
$ |
|
|
|||||||||||||||||||
|
applies to all California building owners and tenants with buildings open to the public. You may obtain information |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
about your legal obligations and how to comply with disability access laws at the following agencies: |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
∙ |
The Division of the State Architect at www.dgs.ca.gov/dsa/Home.aspx. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
∙ |
The Department of Rehabilitation at www.rehab.cahwnet.gov. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
∙ |
The California Commission on Disability Access at www.ccda.ca.gov. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|