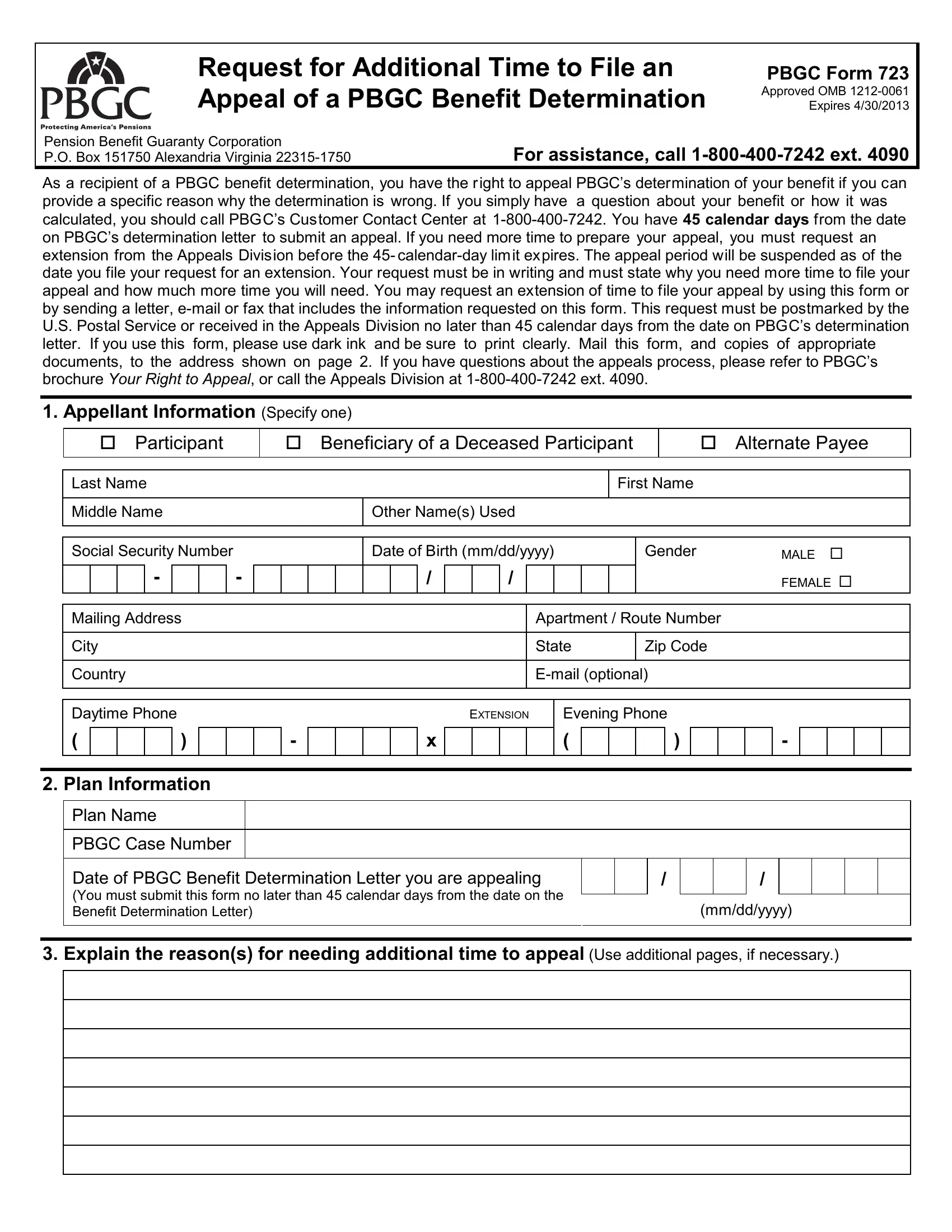
Understanding the nuances of navigating pension benefit appeals with the Pension Benefit Guaranty Corporation (PBGC) can be challenging, especially when seeking additional time to file an appeal. The PBGC Form 723 plays a crucial role in this process, serving as a formal request for extending the filing period for an appeal against a benefit determination. Simply put, if you disagree with how your benefits have been determined by the PBGC, you have a standard 45 calendar days from the receipt of the determination letter to appeal. However, circumstances might not always allow for a prompt response, necessitating the use of Form 723 to request more time. It is essential that such a request outlines the reasons for the delay and specifies the additional time needed. The form can be submitted through various means—mail, email, or fax—and it’s important that it reaches the Appeals Division within the original 45-day timeframe. This form not only signifies the right to contest the PBGC's decision but also emphasizes the importance of ensuring that all procedural steps are meticulously followed to safeguard one's entitlements. Assistance from the PBGC through its customer contact or appeals division is available, reassuring appellants that guidance is at hand throughout this process.
| Question | Answer |
|---|---|
| Form Name | Pbgc Form 723 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | 552a, E-mail, form 723 pbgc, pbgc form 723 |
Request for Additional Time to File an Appeal of a PBGC Benefit Determination
PBGC Form 723
Approved OMB
Pension Benefit Guaranty Corporation
P.O. Box 151750 Alexandria Virginia
For assistance, call
As a recipient of a PBGC benefit determination, you have the right to appeal PBGC’s determination of your benefit if you can provide a specific reason why the determination is wrong. If you simply have a question about your benefit or how it was calculated, you should call PBGC’s Customer Contact Center at
1. Appellant Information (Specify one)
Participant
Beneficiary of a Deceased Participant
Alternate Payee
|
Last Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First Name |
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Middle Name |
|
|
|
|
|
|
|
|
|
Other Name(s) Used |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Social Security Number |
|
|
|
|
|
|
Date of Birth (mm/dd/yyyy) |
|
|
Gender |
|
|
MALE |
||||||||||||||||||||||||||||||
|
|
|
|
- |
|
|
|
|
- |
|
|
|
|
|
|
|
/ |
|
|
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FEMALE |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
Mailing Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
Apartment / Route Number |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State |
|
|
Zip Code |
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Country |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
Daytime Phone |
|
|
|
|
|
|
|
|
|
|
|
|
EXTENSION |
|
Evening Phone |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
( |
|
|
|
|
) |
|
|
|
|
|
|
|
|
x |
|
|
|
|
|
( |
|
|
|
|
|
) |
|
|
|
|
|
- |
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
2. Plan Information |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Plan Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
PBGC Case Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
Date of PBGC Benefit Determination Letter you are appealing |
|
|
|
/ |
|
|
|
|
/ |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
(You must submit this form no later than 45 calendar days from the date on the |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
(mm/dd/yyyy) |
|||||||||||||||||||||||||||||||||||
|
Benefit Determination Letter) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. Explain the reason(s) for needing additional time to appeal (Use additional pages, if necessary.)
Request for Additional Time to File an Appeal of a PBGC Benefit Determination Form 723, page 2 of 2
4. How much additional time do you need to file your appeal?
|
30 days |
45 days |
_____ days (Specify) _________________________ |
|
|
|
|
|
|
5.Authorized Representative Information (if any) If you are representing the Appellant identified in Item 1, select the correct box below and complete the remaining information.
An attorney representing the Appellant
A spouse, family member, or other person assisting the Appellant with this appeal
If you have not already sent PBGC an original notarized power of attorney signed by the Appellant giving you the authority to act on the Appellant’s behalf, you must submit one with this form.
|
Last Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First Name |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Middle Name |
|
|
|
|
|
|
|
Other Name(s) Used |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailing Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
Apartment / Route Number |
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State |
|
Zip Code |
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Country |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Daytime Phone |
|
|
|
|
|
|
|
|
|
EXTENSION |
|
Evening Phone |
|
|
|
|
|
||||||||||||||
|
( |
|
|
|
) |
|
|
|
- |
|
|
|
|
x |
|
|
|
|
( |
|
|
) |
|
|
|
- |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. Signature of Appellant or Authorized Representative – You must sign and date this request. Knowingly and
willfully making false, fictitious or fraudulent statements to the Pension Benefit Guaranty Corporation is a crime punishable under Title 18, Section 1001, United States Code. I declare under penalty of perjury that all of the information I have provided on this form is true and correct to the best of my knowledge.
SIGNATURE |
|
DATE |
HOW TO FILE: You may either mail this completed form, any additional pages and a power of attorney (if
Pension Benefit Guaranty Corporation Attention: Appeals Division
Post Office Box 151750 Alexandria, VA
or, you may fax your request to the Appeals Division at (202)
The Appeals Division will acknowledge your correspondence within one week of receipt. If you have any questions, call the Appeals Division at
PBGC Privacy Act Notice
The Privacy Act of 1974, as amended, 5 U.S.C. § 552a (1994), requires PBGC to give you this notice when collecting information from you. PBGC uses the information to resolve administrative appeals of matters specified in 29 C.F.R. § 4003(b)(5) – (10). Your Social Security Number is used by PBGC to identify your records within PBGC, to report income for tax purposes, and to respond to lawful requests for information about you from other individuals and entities. Your response is voluntary. However, failure to provide information to PBGC, including your Social Security Number, may delay or prevent PBGC from calculating and paying your pension benefits.
The PBGC may release information about you to other individuals and entities when necessary and appropriate under the Privacy Act, including: to a third party who may be aggrieved by a decision of the Appeals Board such as an alternate payee under a qualified domestic relations order; to a third party to make benefit payments to you; or to a labor organization that represents you.
PBGC may also release information about you to appropriate law enforcement agencies when PBGC becomes aware of a possible violation of civil or criminal law. If PBGC, an employee of PBGC, the United States, or another agency of the United States is involved in litigation, PBGC may provide relevant information about you to a court or other adjudicative body or to the Department of Justice when it represents PBGC. PBGC may also provide information about you to the Office of Management and Budget in connection with review of private relief legislation or to a Congressional office in response to an inquiry that office makes about you at your request.
PBGC publishes notices in the Federal Register that describe in more detail when information about you may be made available to others. A copy of the most recent Federal Register notice may be obtained from PBGC's Customer Contact Center by calling
Paperwork Reduction Act Notice
The PBGC needs this information, which is required to be filed under 29 CFR Part 4003, so that it can handle appeals of PBGC initial determinations in certain circumstances. PBGC estimates that it will take an average of 0.75 hours and $55 to comply with these requirements. If you have any comments concerning the accuracy of this estimate or suggestions for improving this form, please send your comments to the Pension Benefit Guaranty Corporation, Legislative and Regulatory Department, 1200 K Street, N.W., Washington, D.C.