
When working in the online PDF tool by FormsPal, you are able to fill out or edit W3 here and now. FormsPal professional team is relentlessly endeavoring to develop the tool and enable it to be even better for people with its cutting-edge functions. Bring your experience one step further with continually improving and exciting possibilities we offer! It merely requires a couple of basic steps:
Step 1: Just hit the "Get Form Button" above on this webpage to start up our pdf file editing tool. This way, you will find all that is needed to fill out your file.
Step 2: When you launch the tool, you will get the form prepared to be completed. Apart from filling in various blanks, you might also do several other actions with the file, specifically adding any words, editing the original textual content, adding illustrations or photos, putting your signature on the form, and much more.
It is straightforward to fill out the document following our helpful guide! Here is what you want to do:
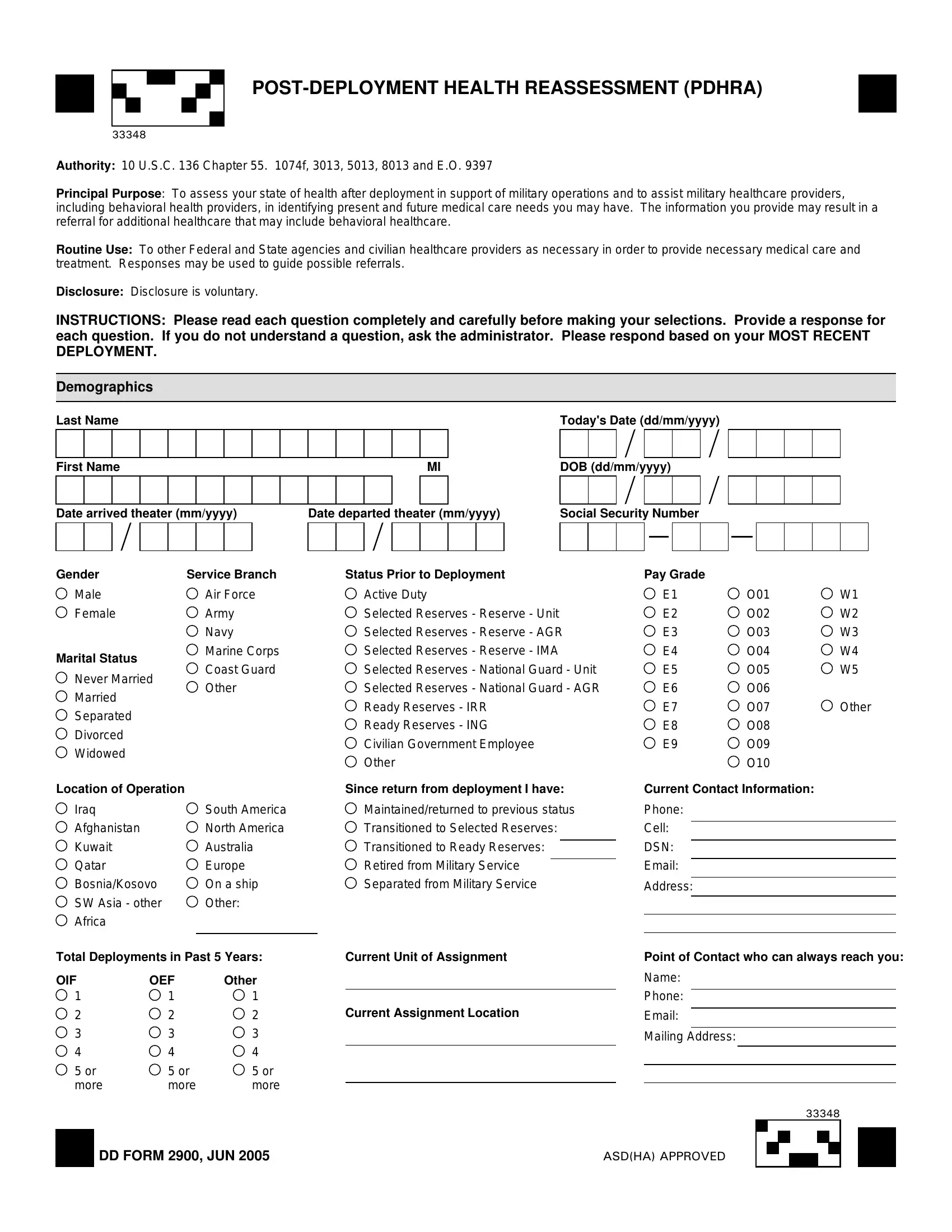
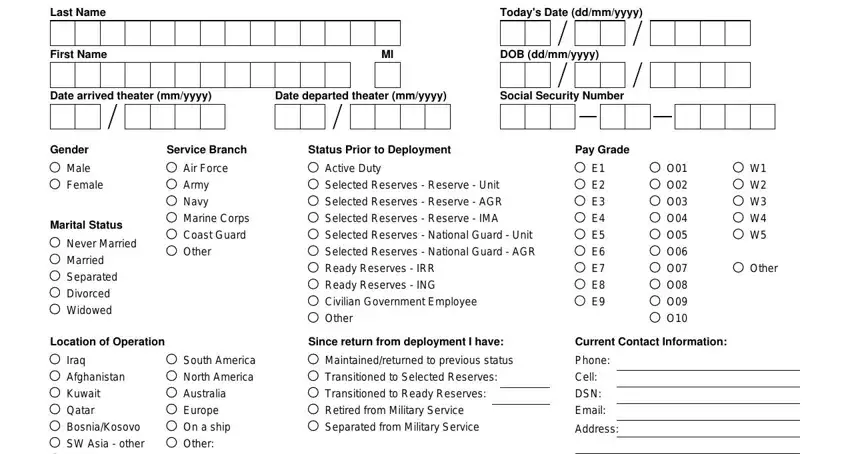
1. To start off, once completing the W3, start with the part that has the next blanks:
2. Your next part is usually to complete these fields: Iraq Afghanistan Kuwait Qatar, Total Deployments in Past Years, Current Unit of Assignment, OIF or more, OEF or more, Other or more, Current Assignment Location, Point of Contact who can always, DD FORM JUN, and ASDHA APPROVED.
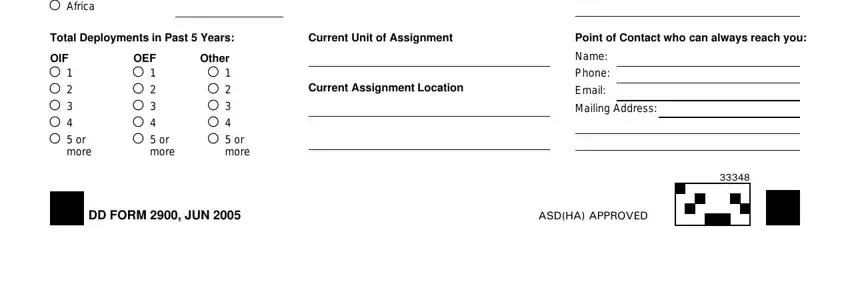
Regarding Total Deployments in Past Years and Current Assignment Location, ensure you don't make any mistakes in this section. The two of these could be the key fields in the PDF.
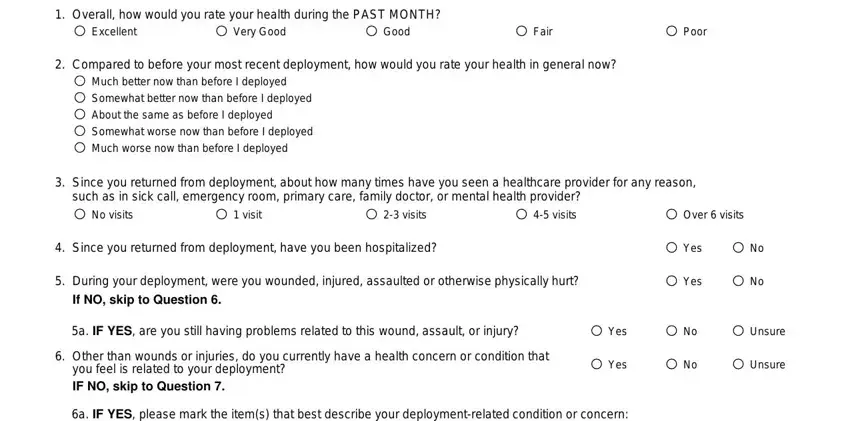
3. Through this step, examine Overall how would you rate your, Excellent, Very Good, Good, Fair, Poor, Compared to before your most, Much better now than before I, Since you returned from, visits, Over visits, No visits, visit, Since you returned from, and During your deployment were you. All of these need to be filled out with highest attention to detail.
4. Completing a IF YES please mark the items, Chronic cough Runny nose Fever, Redness of eyes with tearing, Do you have any persistent major, Yes, a IF YES please mark the items, DEET insect repellent applied to, and Paints Radiation Radarmicrowaves is essential in the fourth section - always spend some time and fill out each field!
5. Finally, the following final portion is what you will need to complete prior to submitting the document. The blank fields in question are the next: DEET insect repellent applied to, DD FORM JUN, Paints Radiation Radarmicrowaves, and Other.
Step 3: Right after you've looked over the details entered, click "Done" to conclude your form. Join FormsPal today and easily gain access to W3, all set for download. All adjustments made by you are kept , letting you change the file at a later time anytime. FormsPal guarantees safe form completion devoid of data recording or sharing. Feel comfortable knowing that your details are safe here!