
Through the online PDF tool by FormsPal, it is possible to fill out or alter pa school health form here. Our expert team is relentlessly endeavoring to develop the editor and ensure it is even faster for people with its multiple features. Enjoy an ever-improving experience today! Getting underway is simple! All you need to do is stick to the following easy steps down below:
Step 1: Open the PDF form inside our editor by clicking on the "Get Form Button" in the top section of this page.
Step 2: With our advanced PDF tool, you're able to do more than just fill in blank form fields. Express yourself and make your forms seem great with custom text incorporated, or modify the file's original input to excellence - all that backed up by an ability to incorporate any photos and sign the document off.
This document will need specific information; in order to ensure accuracy, take the time to pay attention to the next guidelines:
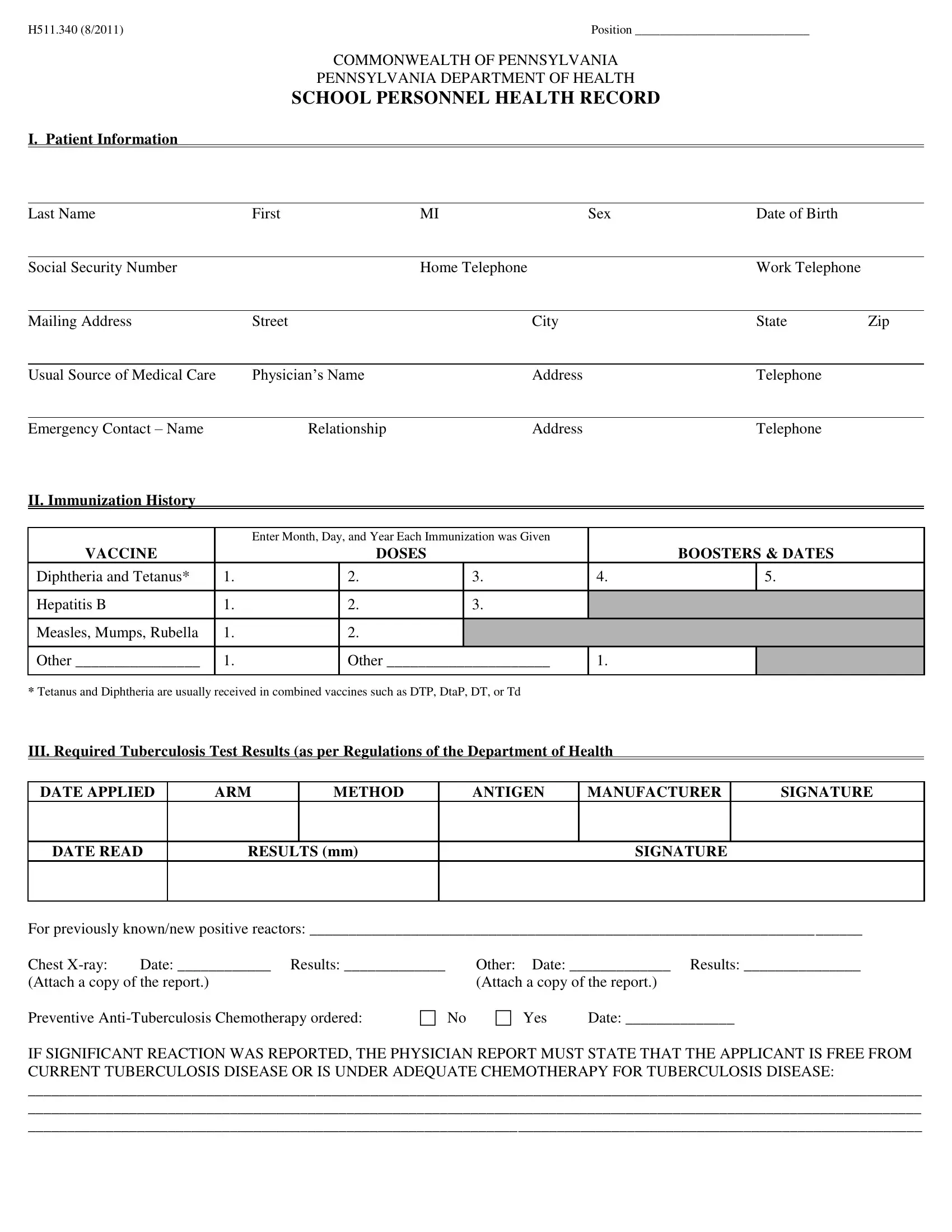
1. The pa school health form requires particular information to be entered. Be sure the following blanks are finalized:
2. Once the previous array of fields is done, you're ready to include the required particulars in VACCINE, Diphtheria and Tetanus, Hepatitis B, Measles Mumps Rubella, Other, Enter Month Day and Year Each, DOSES, BOOSTERS DATES, Other, Tetanus and Diphtheria are, DATE APPLIED, DATE READ, ARM, METHOD, and ANTIGEN so you can proceed to the 3rd stage.
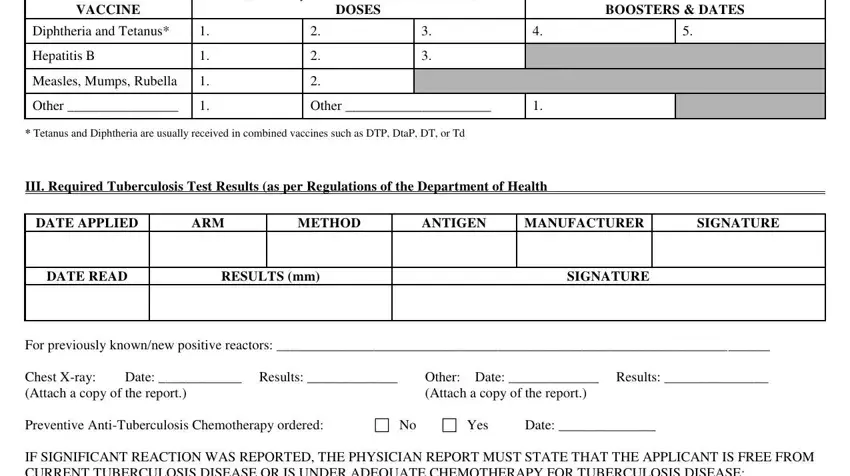
3. The next part should be rather simple, For previously knownnew positive - all of these fields is required to be completed here.

A lot of people frequently make some errors when completing For previously knownnew positive in this part. You need to double-check what you enter here.
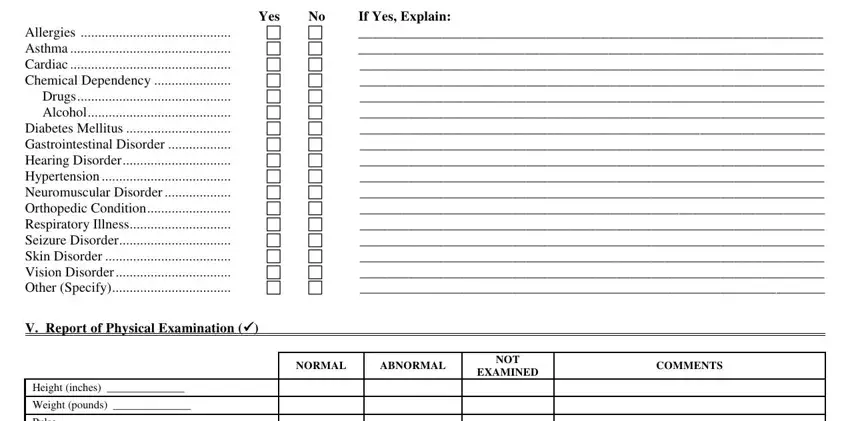
4. This particular section arrives with the next few blank fields to look at: IV Significant Medical Conditions, Yes, If Yes Explain, V Report of Physical Examination, NORMAL, ABNORMAL, NOT, EXAMINED, COMMENTS, Height inches, Weight pounds, and Pulse.
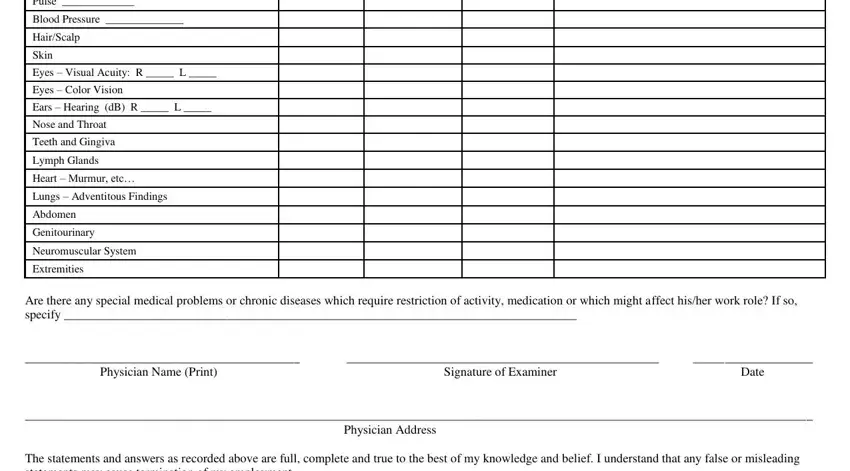
5. Lastly, the following final portion is precisely what you should complete before closing the document. The blanks at issue are the following: Pulse, Blood Pressure, HairScalp, Skin Eyes Visual Acuity R L, Teeth and Gingiva, Lymph Glands Heart Murmur etc, Genitourinary, Neuromuscular System, Extremities, Physician Name Print, Are there any special medical, Signature of Examiner, Date, and Physician Address.
Step 3: Confirm that the information is right and click "Done" to continue further. Create a 7-day free trial account at FormsPal and gain instant access to pa school health form - download or edit in your personal account page. We do not sell or share the details that you type in when filling out documents at FormsPal.