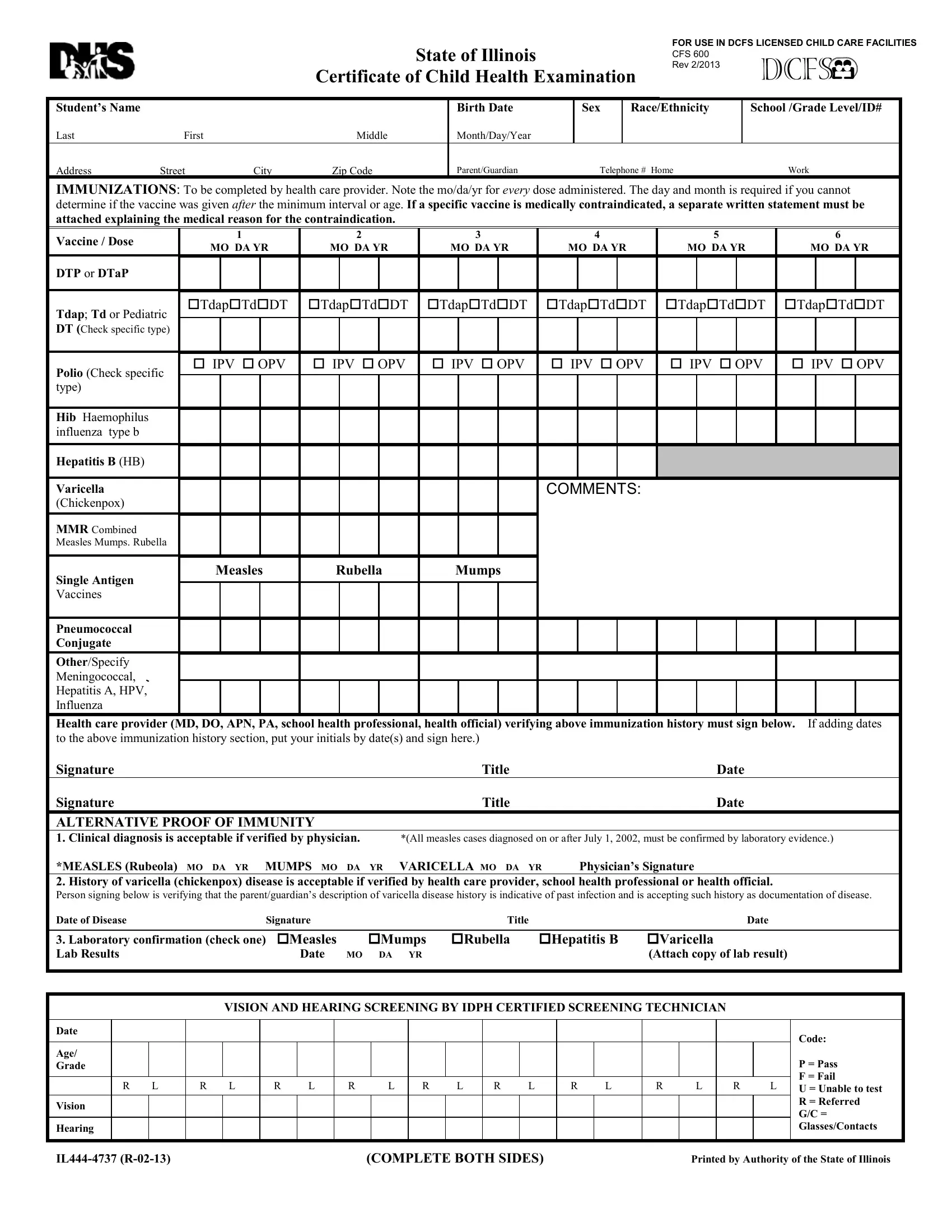
In the State of Illinois, ensuring the well-being and health of children in educational settings is of paramount importance, which is highlighted by the requirement of the Illinois Certificate of Child Health Examination. This comprehensive form, updated and mandated for use in DCFS licensed child care facilities, demands a thorough documentation of a child's immunizations, health history, and screenings for vision and hearing. It requires detailed records of vaccinations against a number of diseases, with space to note any medical contraindications and alternative proofs of immunity where applicable. Beyond immunizations, the form delves into the child's medical history, including allergies, medications, surgeries, and any diagnoses of chronic conditions like asthma or diabetes, as well as noting any developmental delays or physical disabilities. Vision and hearing screenings are integral parts of the examination, ensuring any issues that could affect the child's learning are identified early. Additionally, the form addresses the need for diabetes screening in certain at-risk populations and contains a lead risk questionnaire mandatory for young children in specific areas or circumstances. The exhaustive nature of this health examination form ensures that educators, healthcare providers, and guardians are all aligned in their understanding of a child's health needs and conditions, facilitating a supportive and safe educational environment.
| Question | Answer |
|---|---|
| Form Name | Illinois Child Health Examination Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | certificate of child health examination, state of illinois certificate of child health examination 2021, illinois physical exam form, illinois physical exam |