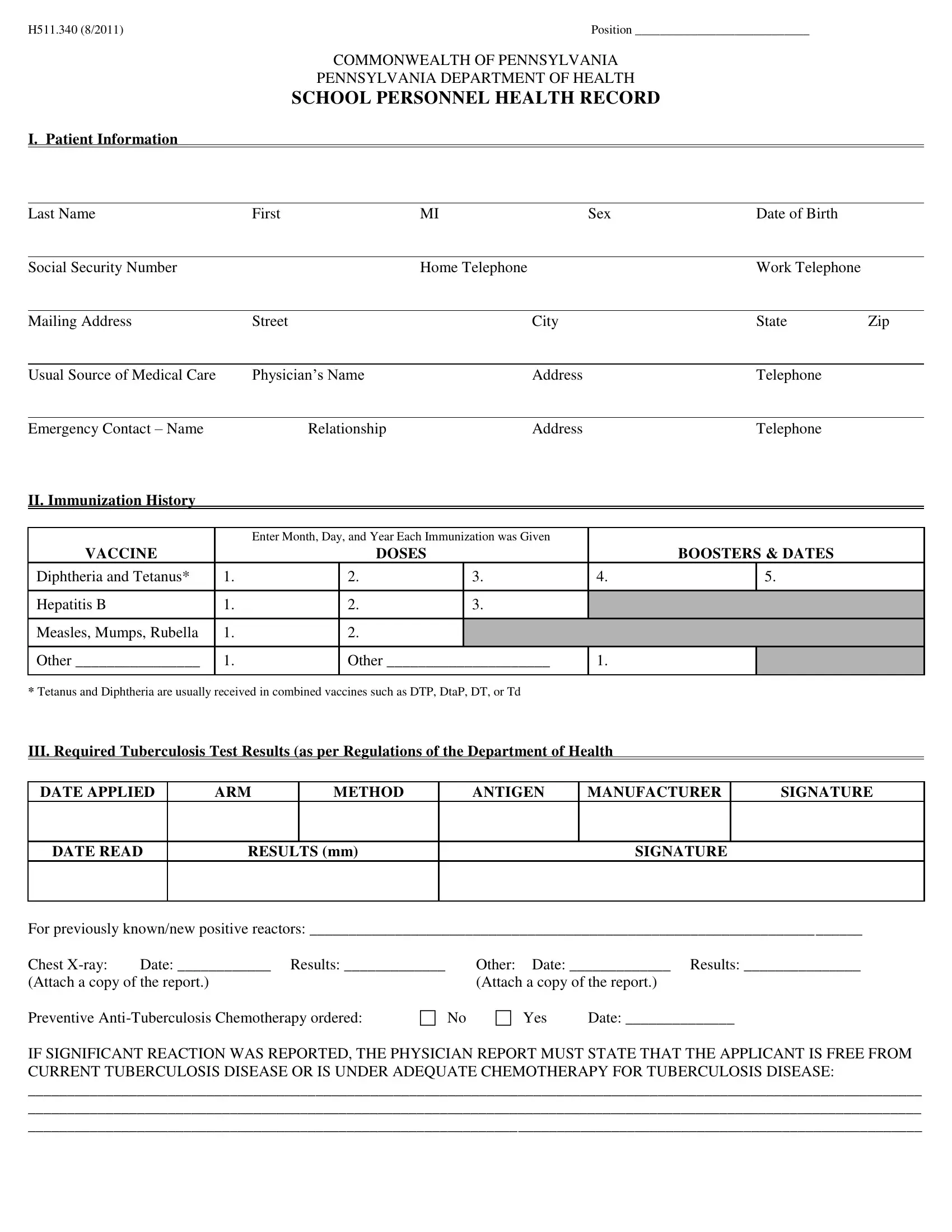
In the Commonwealth of Pennsylvania, the Pennsylvania Department of Health has designated a comprehensive form, known as H511.340 (8/2011), to streamline the process of monitoring and documenting the health status of school personnel. This meticulous form captures a wide array of essential health information beginning with basic patient identification details including name, contact information, and the patient's primary care provider. It extends to cover a detailed immunization history, specifying doses and booster shots for vaccines such as Diphtheria, Tetanus, Hepatitis B, and Measles, Mumps, Rubella among others. The form also places a significant emphasis on tuberculosis testing, outlining the procedure for reporting the test results and subsequent actions in the event of positive reactions. Additionally, it dives deep into identifying significant medical conditions across a broad spectrum including allergies, asthma, cardiac issues, and more, ensuring each is noted with the option to provide detailed explanations. The physical examination report section further scrutinizes various health aspects, from basic measurements to comprehensive evaluations of bodily systems, aiming to identify conditions that may affect the work role of the school personnel. Among its final stipulations, the form requires an acknowledgment by the personnel of the completeness and truthfulness of the provided information, coupled with a consent for the disclosure of this health data to the employing authority. This well-structured health form stands as a critical tool in managing and ensuring the well-being and fitness of individuals within the school environment.
| Question | Answer |
|---|---|
| Form Name | Pennsylvania Health Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | school personnel health record, pennsylvania school health form, pa school health form, pa school personnel health form |