Ensuring the safety of individuals handling pesticides is a paramount concern for employers in agricultural and related industries. The Pesticide Safety Training form plays a critical role in this process, providing a comprehensive record of training sessions that cover vital safety protocols and procedures. The form documents the engagement of employees in a Pesticide Handler Training Program, including their names, signatures, and details of the trainers responsible for the sessions. It covers a range of assigned job duties, such as mixer/loader, applicator, and repair services, ensuring that each worker is adequately trained according to their role. Crucially, the form outlines key subjects mandated by the California Code of Regulations, such as understanding labels, knowing the required protective clothing and equipment, and recognizing the symptoms of poisoning. It emphasizes the importance of cleanliness, the correct use of engineering controls, emergency procedures, and the medical supervision required for certain pesticide handlers. This document not only serves as a testament to an employer’s commitment to regulatory compliance but, more importantly, as a crucial tool in safeguarding the health and safety of individuals exposed to pesticide-related risks.
| Question | Answer |
|---|---|
| Form Name | Pesticide Safety Training Form |
| Form Length | 10 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 2 min 30 sec |
| Other names | pesticide training safety, pesticide handler program, pesticide safety training handler, pesticide safety training record form |
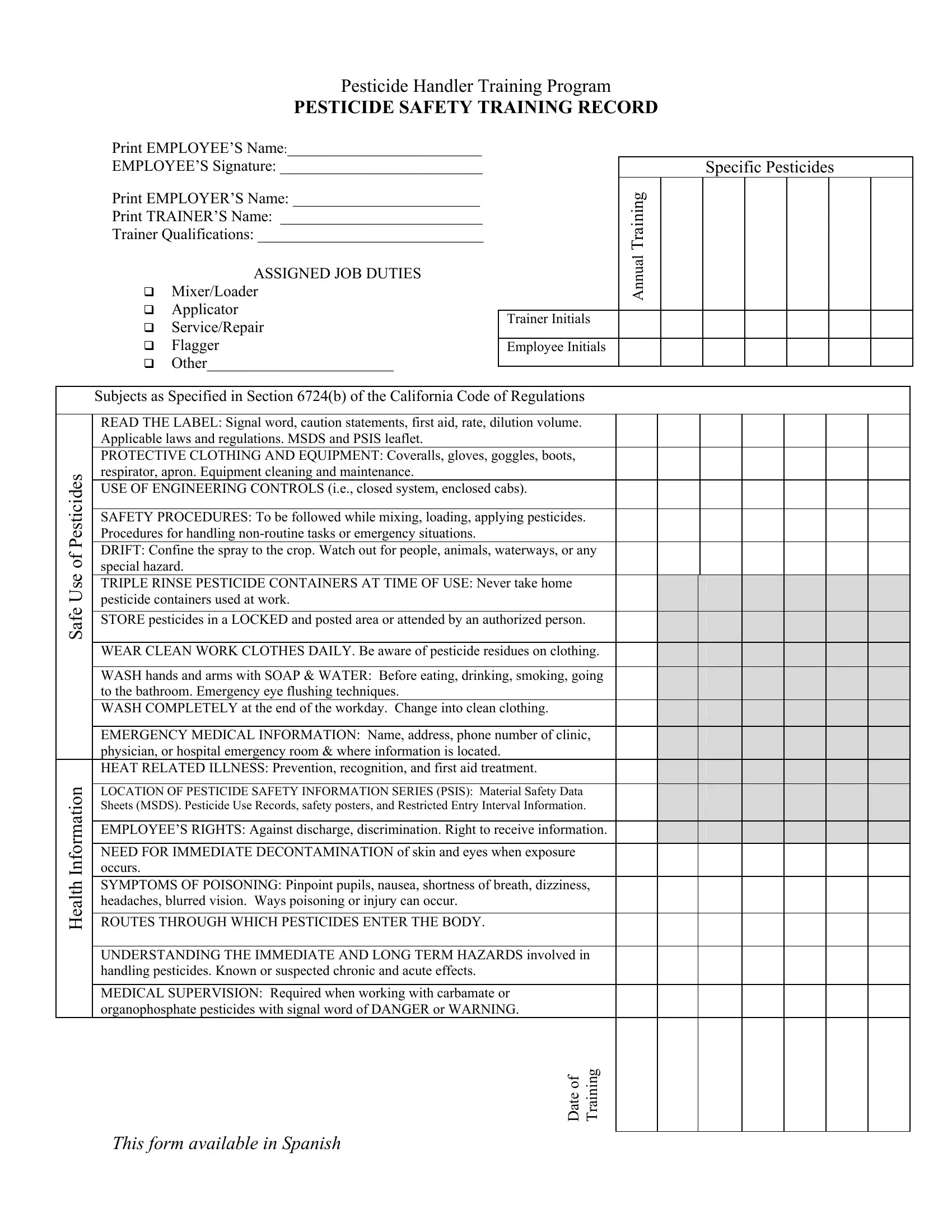
Pesticide Handler Training Program
PESTICIDE SAFETY TRAINING RECORD
Print EMPLOYEE’S Name:_________________________
EMPLOYEE’S Signature: __________________________
Print EMPLOYER’S Name: ________________________
Print TRAINER’S Name: __________________________
Trainer Qualifications: _____________________________
|
ASSIGNED JOB DUTIES |
|
|||
|
Mixer/Loader |
|
|||
|
Applicator |
|
|
Trainer Initials |
|
|
|
||||
|
Service/Repair |
|
|
||
|
|
|
|
||
|
Flagger |
|
|
Employee Initials |
|
|
Other________________________ |
|
|
|
|
|
|
|
|||
|
Subjects as Specified in Section 6724(b) of the California Code of Regulations |
||||
|
READ THE LABEL: Signal word, caution statements, first aid, rate, dilution volume. |
||||
|
|||||
|
Applicable laws and regulations. MSDS and PSIS leaflet. |
|
|||
|
PROTECTIVE CLOTHING AND EQUIPMENT: Coveralls, gloves, goggles, boots, |
||||
Pesticides |
respirator, apron. Equipment cleaning and maintenance. |
|
|||
USE OF ENGINEERING CONTROLS (i.e., closed system, enclosed cabs). |
|||||
|
|||||
|
SAFETY PROCEDURES: To be followed while mixing, loading, applying pesticides. |
||||
|
Procedures for handling |
|
|||
of |
DRIFT: Confine the spray to the crop. Watch out for people, animals, waterways, or any |
||||
special hazard. |
|
||||
Use |
|
||||
TRIPLE RINSE PESTICIDE CONTAINERS AT TIME OF USE: Never take home |
|||||
|
|||||
Safe |
pesticide containers used at work. |
|
|||
STORE pesticides in a LOCKED and posted area or attended by an authorized person. |
|||||
|
|||||
|
WEAR CLEAN WORK CLOTHES DAILY. Be aware of pesticide residues on clothing. |
||||
|
WASH hands and arms with SOAP & WATER: Before eating, drinking, smoking, going |
||||
|
to the bathroom. Emergency eye flushing techniques. |
|
|||
|
WASH COMPLETELY at the end of the workday. Change into clean clothing. |
||||
|
EMERGENCY MEDICAL INFORMATION: Name, address, phone number of clinic, |
||||
|
physician, or hospital emergency room & where information is located. |
|
|||
Information |
HEAT RELATED ILLNESS: Prevention, recognition, and first aid treatment. |
||||
occurs. |
|
||||
|
LOCATION OF PESTICIDE SAFETY INFORMATION SERIES (PSIS): Material Safety Data |
||||
|
Sheets (MSDS). Pesticide Use Records, safety posters, and Restricted Entry Interval Information. |
||||
|
EMPLOYEE’S RIGHTS: Against discharge, discrimination. Right to receive information. |
||||
|
NEED FOR IMMEDIATE DECONTAMINATION of skin and eyes when exposure |
||||
Health |
SYMPTOMS OF POISONING: Pinpoint pupils, nausea, shortness of breath, dizziness, |
||||
ROUTES THROUGH WHICH PESTICIDES ENTER THE BODY. |
|
||||
|
headaches, blurred vision. Ways poisoning or injury can occur. |
|
|||
|
UNDERSTANDING THE IMMEDIATE AND LONG TERM HAZARDS involved in |
||||
|
handling pesticides. Known or suspected chronic and acute effects. |
|
|||
|
MEDICAL SUPERVISION: Required when working with carbamate or |
||||
|
organophosphate pesticides with signal word of DANGER or WARNING. |
||||
Specific Pesticides
Annual Training
Date of Training
This form available in Spanish
Pesticide Handler Training Program
DATOS DE ENTRENAMIENTO DE SEGURIDAD PARA EL USO DE PESTICIDAS
Nombre de EMPLEADO: ________________________
Firma de EMPLEADO: _________________________
Nombre de MAYORDOMO:_____________________
Nombre de ENTRENADOR:_____________________
Títulos de ENTRENADOR:______________________
TRABAJO ASIGNADO
Mezclador/Cargador
Aplicador/rociador
Mantenimiento/Reparación
Banderero
Otro________________________
Iniciales del Entrenador
Iniciales del Empleado
Pesticidas Especificas
Entrenamiento |
Anual |
Subjects as Specified in Section 6724 (b) of the California Code of Regulations
Uso Seguro de Pesticidas
Información de Salud
Lea la etiqueta: Palabras señales, declaraciones de precauciones, primeros auxilios, dosis, dilución, volumen. Leyes y reglamentos aplicables, MSDS, y hojas de PSIS.
Ropa y equipo protector (sobreropa, guantes, gafas, botas de hule, respirador, delantal) Limpieza y mantenimiento de equipo.
Uso de controles de ingeniería como sistemas cerrados o cabinas cerradas.
Procedimientos de seguro que debe usar cuando mezclando, cargando, o aplicando pesticidas. Situaciones de emergencia.
Deriva: Limite el rocío a la cosecha. Tenga cuidado con la gente, animales, vías de aguas, o cualquier peligro especial.
Enjuague los envases tres veces en tiempo de uso. Nunca se lleve envases de pesticidas usadas en su trabajo para su casa.
Use ropa de trabajo limpia diariamente. Darse cuenta de residuos de pesticidas en su ropa.
Los envases de pesticidas deben estar en un almacenaje con candado y rótulos o con una persona autorizada cuidando los.
Lave las manos y brazos con agua y jabón: Antes de comer, beber, fumar e ir al baño. Técnicas de emergencia para enjuagarse los ojos.
Lavarse completamente al fin del día de trabajo: Cambiarse a ropa limpia.
Donde buscar atención medica en emergencia: Nombre, domicilio, numero de teléfono de la clínica, doctor, o cuarto de emergencia del hospital.
Prevención, reconocimiento, primeros auxilios y tratamiento de enfermedad relacionada al calor.
Localización de la Serie de Información de Seguridad con Pesticidas (PSIS) o hojas de seguridad de producto (MSDS), archivos de aplicaciones de pesticidas, letreros de seguridad, y intervalos restringidos de reingreso (REI).
Derechos del empleado: contra descarga, discriminación y derechos de recibir información.
La necesidad para decontaminación inmediatamente de la piel y los ojos cuando sucede exposición.
Síntomas de envenenamiento: Pupilas muy pequeñas, nauseas, respiración breve, vértigo, dolor de cabeza, visión borrosa. Modo como envenenamiento o lesión puede ocurrir.
Rutas a través como pesticidas pueden entrar al cuerpo: boca, piel, ojos, inhalación.
Entendimiento de los peligros del uso de pesticidas inmediatos y de largo plazo; los efectos sospechosos o conocidos agudos o crónicos.
Supervisión medica: Requerido si trabaja mas de 6 días en 30 días con carbamatos, organofosfatos con las palabras “PELIGRO” o “AVISO” en la etiqueta.
Entrenamiento
Fecha De
Medical Supervision Program
EMPLOYEE PESTICIDE USE RECORD
Employee Name: __________________________________________________________
Whenever an employee mixes, loads, or applies a DANGER or WARNING pesticide that contains an organophosphate or carbamate, the employer must maintain use records that identify the employee, name of pesticide, and date of use. Retain these records for three years.
Date of Use
Pesticide Name
Signal Word
Carbamate/
Organophosphate
FIELDWORKER SAFETY TRAINING RECORD
NAME OF EMPLOYER: ______________________________DATE:_________________
NAME OF TRAINER: _______________________________________________________
Trainer’s qualification: ________________________________________________________
Symptoms of poisoning: Pinpoint pupils, nausea |
|
Location of pesticide safety information series (PSIS) |
|
shortness of breath, dizziness, blurred vision. Ways |
|
Material safety data sheets (MSDS), pesticide use |
|
poisoning or injury can occur. |
|
reports, safety posters, and restricted entry intervals. |
|
|
|
|
|
Wash hands and arms with soap and water: Before |
|
The need for immediate decontamination of skin and |
|
eating drinking, smoking, or going to the bathroom. |
|
eyes when exposure occurs. |
|
Emergency Eye flushing techniques. |
|
|
|
|
|
|
|
Wash completely at the end of the workday and |
|
Employee’s rights: against discharge, discrimination, |
|
change into clean clothing. |
|
rights to receive information. |
|
|
|
|
|
Wear clean work clothing daily. Be aware of |
|
Routes through which pesticides enter the body. |
|
pesticides residues on clothing. |
|
|
|
|
|
|
|
Understanding the immediate and |
|
Prevention, recognition, and first aid treatment of heat |
|
involved in handling pesticides. Known or |
|
related illness. |
|
suspected chronic and acute effects. |
|
|
|
|
|
|
|
Emergency medical information: Name, address, |
|
Restricted entry intervals and posting. Do not enter |
|
phone number of clinic, physician, or hospital |
|
treated areas. |
|
emergency room and where information is located. |
|
|
|
|
|
|
|
Never take home pesticide containers used at work. |
|
|
|
|
|
|
|
Print Your Name |
Sign Your Name |
1. _________________________________ |
______________________________ |
2. _________________________________ |
______________________________ |
3. _________________________________ |
______________________________ |
4. _________________________________ |
______________________________ |
5. _________________________________ |
______________________________ |
6. _________________________________ |
______________________________ |
7. _________________________________ |
______________________________ |
8. _________________________________ |
_______________________________ |
|
This form available in Spanish |
ARCHIVO DE ENTRENAMIENTO DE PESTICIDAS
PARA CAMPESIONS
NOMBRE DE PATRON: ______________________________FECHA: ___________________
NOMBRE DE ENTREADOR: ____________________________________________________
CALIFICACIONES DE LENTRENADOR: ___________________________________________
Síntomas de envenenamiento: Pupilas muy pequeñas, |
|
Localización de Serie de Información de Seguridad con |
|
nauseas, vértigo, dolor de cabeza, visión borrosa, |
|
Pesticidas (PSIS) o hojas de seguridad de producto (MSDS) , |
|
respiración breve. Modo en envenenamiento o lesión |
|
archivos de aplicaciones de pesticidas, letreros de seguridad, y |
|
puede ocurrir. |
|
intervalos restringidos de reingreso (REI). |
|
Lave las manos y brazos con agua y jabón: Antes de |
|
La necesidad para decontaminación inmediatamente de la piel |
|
comer, beber, fumar y ir al baño. Técnicas de emergencia |
|
y los ojos cuando sucede exposición. |
|
para enjuagarse los ojos. |
|
|
|
|
|
|
|
Lavarse completamente al fin del día de trabajo: |
|
Derechos del empleado: contra descarga, discriminación y |
|
|
derechos de recibir información. |
|
|
Cambiarse a ropa limpia. |
|
|
|
|
|
|
|
|
|
|
|
Use ropa de trabajo limpia diariamente. Darse cuenta de |
|
Rutas a través como pesticidas pueden entrar al cuerpo: boca, |
|
residuos de pesticidas en su ropa. |
|
piel, ojos, inhalación. |
|
|
|
|
|
Entendimiento de los peligros del uso de pesticidas |
|
Prevención, reconocimiento, primeros auxilios y tratamiento de |
|
inmediatos y de largo plazo; los efectos sospechosos o |
|
enfermedad relacionada al calor. |
|
conocidos agudos o crónicos. |
|
|
|
|
|
|
|
Donde buscar atención medica en emergencia: Nombre, |
|
Intervalos de entrada restringidos (REI) y letreros de REI. No |
|
domicilio, numero de teléfono de la clínica, doctor, o |
|
entre a una área tratada. |
|
cuarto de emergencia del hospital. |
|
|
|
|
|
|
|
Nunca se lleve envases de pesticidas usadas en su trabajo |
|
|
|
para su casa. |
|
|
|
|
|
|
|
Escriba su Nombre en Letra de Molde |
|
Firma |
|
1. _________________________________ |
______________________________ |
|
|
2. _________________________________ |
______________________________ |
|
|
3. _________________________________ |
______________________________ |
|
|
4. _________________________________ |
______________________________ |
|
|
5. _________________________________ |
______________________________ |
|
|
6. _________________________________ |
______________________________ |
|
|
7. _________________________________ |
______________________________ |
|
|
8. _________________________________ |
_______________________________ |
|
|
9. _________________________________ |
_______________________________ |
|
|
Medical Supervision Program
MEDICAL SUPERVISION WRITTEN AGREEMENT
I, ___________________________(Physician name), agree to provide medical supervision for
the employees of __________________________________________.
(Grower or Company)
I possess a copy of, and am aware of the contents of, the following documents:
Medical Supervision of Pesticide Workers - Guidelines for Physicians.
____________________________________________
(Physician)
____________________________________________
(Address)
____________________________________________
(City, State, Zip)
____________________________________________
(Telephone)
____________________________________________
(Signed)
___________________________________________
(Grower Name/Company)
___________________________________________
(Address)
___________________________________________
(City, State, Zip)
__________________________________________
(Telephone)
__________________________________________
(Signed)
WRITTEN TRAINING PROGRAM
Employer Name: _________________________________________________
Trainer’s Name: _________________________________________________
Trainer’s Qualification: _________ PA: _________ QAL/QAC: _________ PCA: _________
Training Materials:
Name of videos, pamphlets, or other training materials, and a brief description:
1.______________________________________________________________________
2.______________________________________________________________________
3.______________________________________________________________________
4.______________________________________________________________________
Pesticide labeling from the following products:
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
Pesticide Safety Information Series (PSIS) leaflets used:
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
Materials Safety Data Sheets (MSDS) for the following products:
________________________________________________________________________
________________________________________________________________________
_________________________________________________________________________
LETTER OF AUTHORIZATION
To: _______________________________________, County Agricultural Commissioner
From: ________________________________________________________________________
OPERATOR OF THE PROPERTY (PRINT NAME)
_____________________________________________________________________________
ADDRESS
_____________________________________________________________________________
CITY, STATE, ZIP, PHONE
The authorized representative named below may represent me in obtaining a restricted material permit or operator identification number for use in ___________________County. I understand
that this authorization does not relieve me of liability for violations of pesticide laws or regulations on my property. This authorization shall remain in effect until I revoke it in writing to the Agricultural Commissioner.
Signature: __________________________________________ Date: _____________________
(OPERATOR OF THE PROPERTY)
Title: ________________________________________________________________________
Authorized Representative: _______________________________________________________
(PRINT NAME)
I am the property operator’s: [ ] employee; [ ] relative; [ ] employee PCA;
[ ] other, SPECIFY_______________________
I hereby certify that the information above is correct to the best of my knowledge. I also understand that, in the event of violation of pesticide laws or regulations, I could be held liable either separately or together with the property operator.
Signed: _______________________________________________ Phone: _________________
AUTHORIZED REPRESENTATIVE
3CCR 6420(a): “Permits for agricultural use of a restricted material shall be issued in the name of the operator of the property to be treated. The permittee or, when allowed by the commissioner, the permittee’s authorized representative or licensed pest control adviser shall sign the permit. The authorized representative or licensed pest control adviser shall provide the commissioner with written documentation from the permittee to act on his/her behalf.”
3CCR 6000: “Operator of the property” means a person who owns the property and/or is legally entitled to possess or use the property through terms of a lease, rental contract, trust, or other management arrangement.

|
|
|
Restricted |
|
|
Pesticide |
Location |
Date/Time |
Entry |
Active ingredient |
Registration |
|
|
|
Interval |
|
Number |
|
|
|
(REI) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Complete chart within 24 hours of the application and display where employees can review the information with unimpeded access.

Product active ingredients and EPA Registration numbers are found on the labels displayed with this chart.
Pesticide |
Location |
Date/Time |
Restricted |
|
|
|
Entry Interval |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Complete chart within 24 hours of the application and display with the pesticide labels used where employees can review the information with unimpeded access.