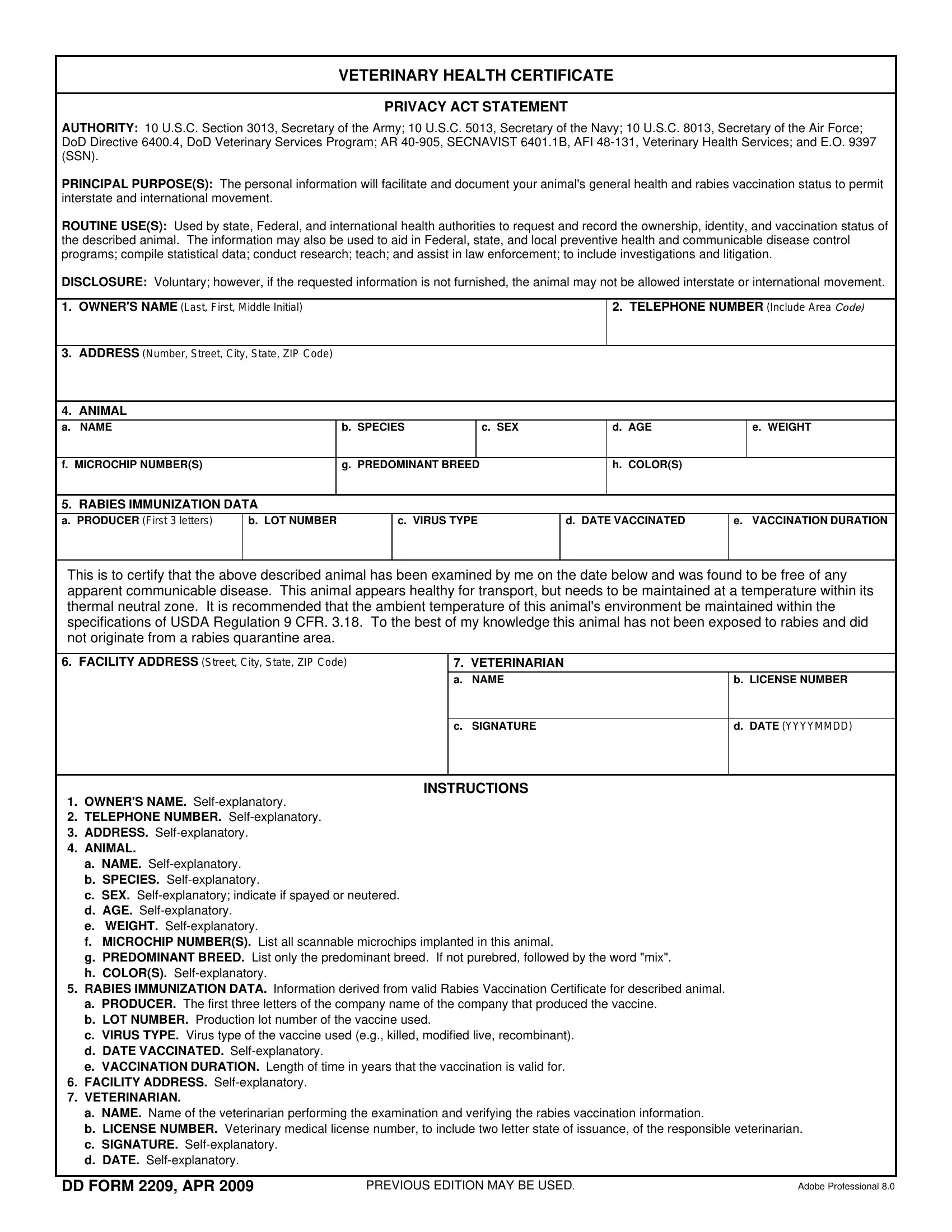
VETERINARY HEALTH CERTIFICATE
PRIVACY ACT STATEMENT
AUTHORITY: 10 U.S.C. Section 3013, Secretary of the Army; 10 U.S.C. 5013, Secretary of the Navy; 10 U.S.C. 8013, Secretary of the Air Force; DoD Directive 6400.4, DoD Veterinary Services Program; AR 40-905, SECNAVIST 6401.1B, AFI 48-131, Veterinary Health Services; and E.O. 9397 (SSN).
PRINCIPAL PURPOSE(S): The personal information will facilitate and document your animal's general health and rabies vaccination status to permit interstate and international movement.
ROUTINE USE(S): Used by state, Federal, and international health authorities to request and record the ownership, identity, and vaccination status of the described animal. The information may also be used to aid in Federal, state, and local preventive health and communicable disease control programs; compile statistical data; conduct research; teach; and assist in law enforcement; to include investigations and litigation.
DISCLOSURE: Voluntary; however, if the requested information is not furnished, the animal may not be allowed interstate or international movement.
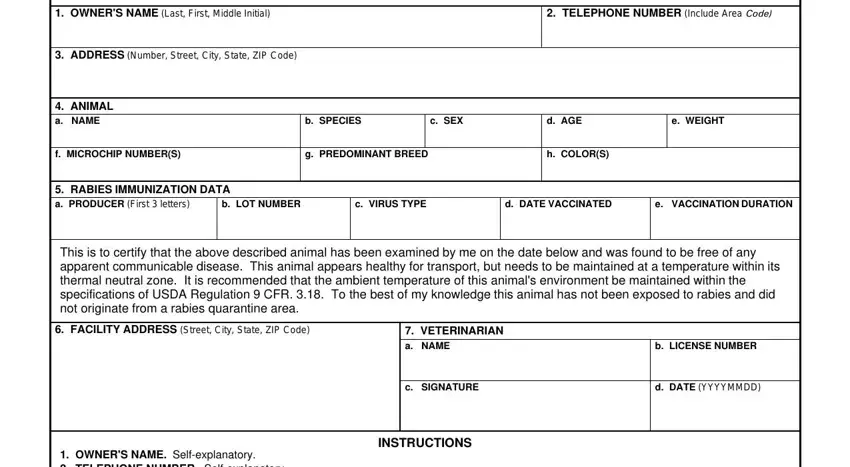
1. OWNER'S NAME (Last, First, Middle Initial)
2. TELEPHONE NUMBER (Include Area Code)
3.ADDRESS (Number, Street, City, State, ZIP Code)
4.ANIMAL
a. NAME |
b. |
SPECIES |
|
c. SEX |
d. |
AGE |
e. WEIGHT |
|
|
|
|
|
|
|
|
f. MICROCHIP NUMBER(S) |
g. |
PREDOMINANT BREED |
|
h. |
COLOR(S) |
|
|
|
|
|
|
|
|
|
5. RABIES IMMUNIZATION DATA
a.PRODUCER (First 3 letters)
This is to certify that the above described animal has been examined by me on the date below and was found to be free of any apparent communicable disease. This animal appears healthy for transport, but needs to be maintained at a temperature within its thermal neutral zone. It is recommended that the ambient temperature of this animal's environment be maintained within the specifications of USDA Regulation 9 CFR. 3.18. To the best of my knowledge this animal has not been exposed to rabies and did not originate from a rabies quarantine area.
6.FACILITY ADDRESS (Street, City, State, ZIP Code)
7. VETERINARIAN
a. NAME |
b. LICENSE NUMBER |
INSTRUCTIONS
1.OWNER'S NAME. Self-explanatory.
2.TELEPHONE NUMBER. Self-explanatory.
3.ADDRESS. Self-explanatory.
4.ANIMAL.
a.NAME. Self-explanatory.
b.SPECIES. Self-explanatory.
c.SEX. Self-explanatory; indicate if spayed or neutered.
d.AGE. Self-explanatory.
e.WEIGHT. Self-explanatory.
f.MICROCHIP NUMBER(S). List all scannable microchips implanted in this animal.
g.PREDOMINANT BREED. List only the predominant breed. If not purebred, followed by the word "mix".
h.COLOR(S). Self-explanatory.
5.RABIES IMMUNIZATION DATA. Information derived from valid Rabies Vaccination Certificate for described animal.
a.PRODUCER. The first three letters of the company name of the company that produced the vaccine.
b.LOT NUMBER. Production lot number of the vaccine used.
c.VIRUS TYPE. Virus type of the vaccine used (e.g., killed, modified live, recombinant).
d.DATE VACCINATED. Self-explanatory.
e.VACCINATION DURATION. Length of time in years that the vaccination is valid for.
6.FACILITY ADDRESS. Self-explanatory.
7.VETERINARIAN.
a.NAME. Name of the veterinarian performing the examination and verifying the rabies vaccination information.
b.LICENSE NUMBER. Veterinary medical license number, to include two letter state of issuance, of the responsible veterinarian.
c.SIGNATURE. Self-explanatory.
d.DATE. Self-explanatory.
DD FORM 2209, APR 2009 |
PREVIOUS EDITION MAY BE USED. |
ADobe Professional 8.0 |