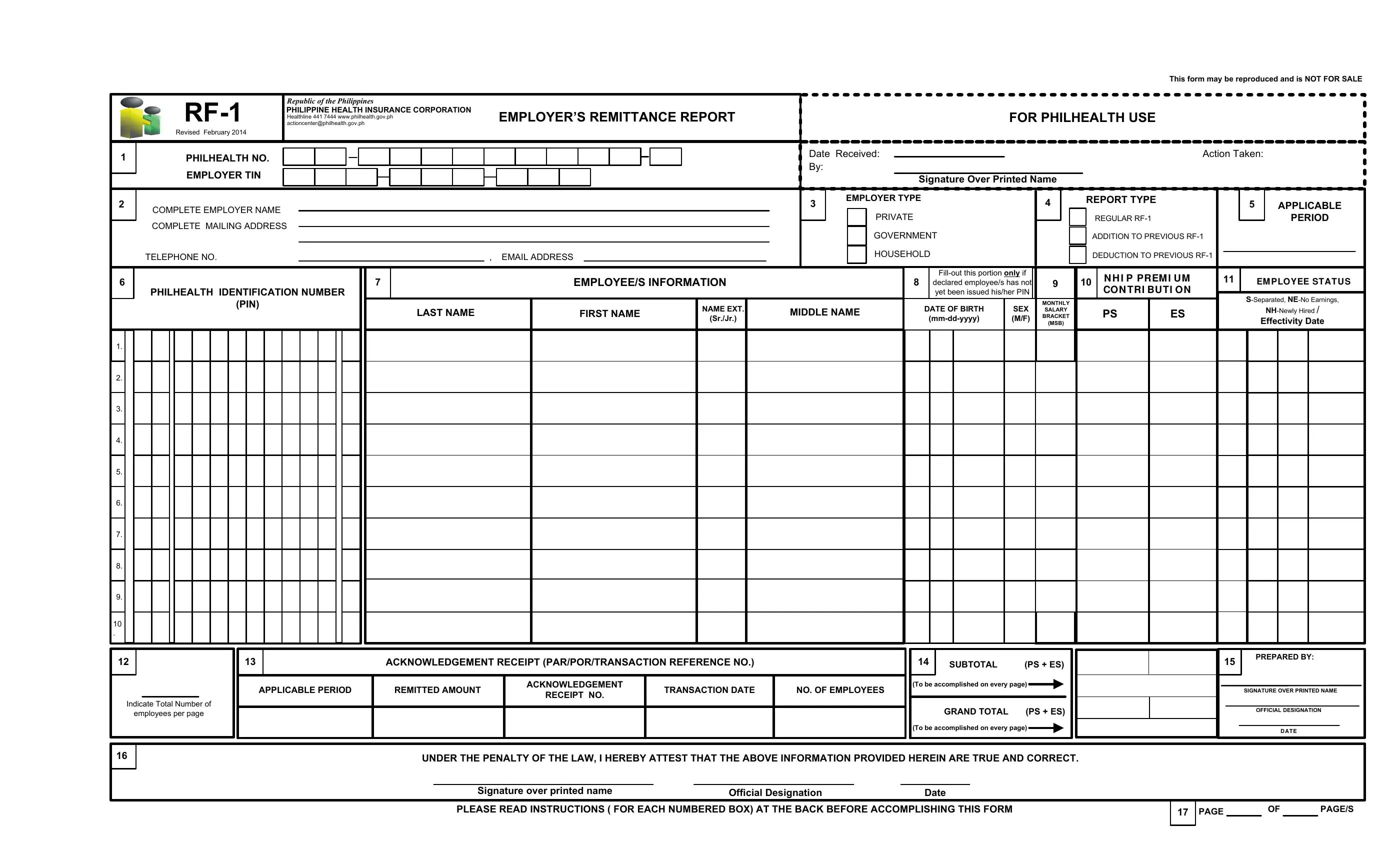
Navigating the complexities of health insurance contributions in the Philippines is made more manageable with the RF-1 form provided by the Philippine Health Insurance Corporation (PhilHealth). This essential document, designed for employers, ensures the accurate reporting and remittance of their employees' health premiums. It encompasses detailed sections for employer and employee information, including tax identification numbers, types of employment, and detailed salary brackets that correspond to specific premium contributions. The form also offers guidance for adjustments related to past remittances and provides a system for identifying employees through their PhilHealth Identification Numbers. Monthly salary brackets are clearly outlined to facilitate the correct computation of contributions, divided equally between employer and employee. Moreover, the form outlines the responsibilities of employers in case of discrepancies or failures in remittance, emphasizing the legal implications and the importance of timely and correct submissions. With its revision in February 2014, the RF-1 form aligns with the efforts of the Philippine government to streamline processes and ensure that every Filipino employee is adequately covered by health insurance.
| Question | Answer |
|---|---|
| Form Name | Ph Rf 1 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | downloadable blank philhealth id template, rf1 excel format, rf1, philhealth id editor |
