 Bangsamoro/Normalization
Bangsamoro/Normalization
 Point of Service (POS) Financially Incapable
Point of Service (POS) Financially Incapable 
 Financially Incapable
Financially Incapable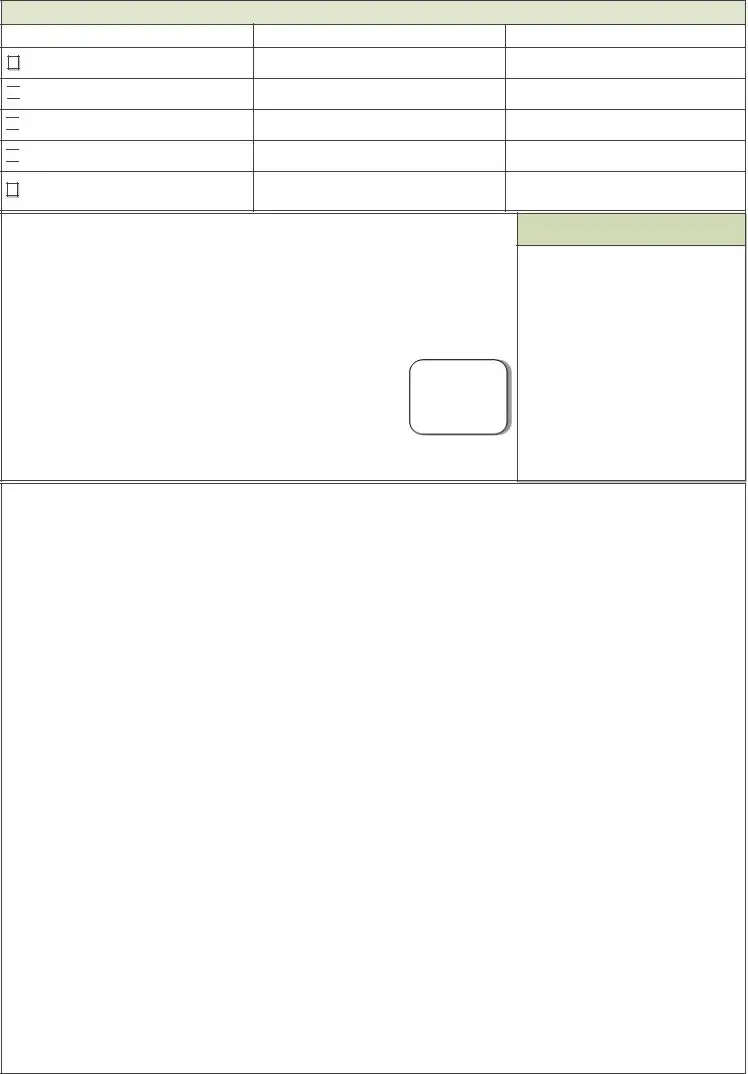

 Correction of Date of Birth
Correction of Date of Birth
 Correction of Sex
Correction of Sex
 Change of Civil Status
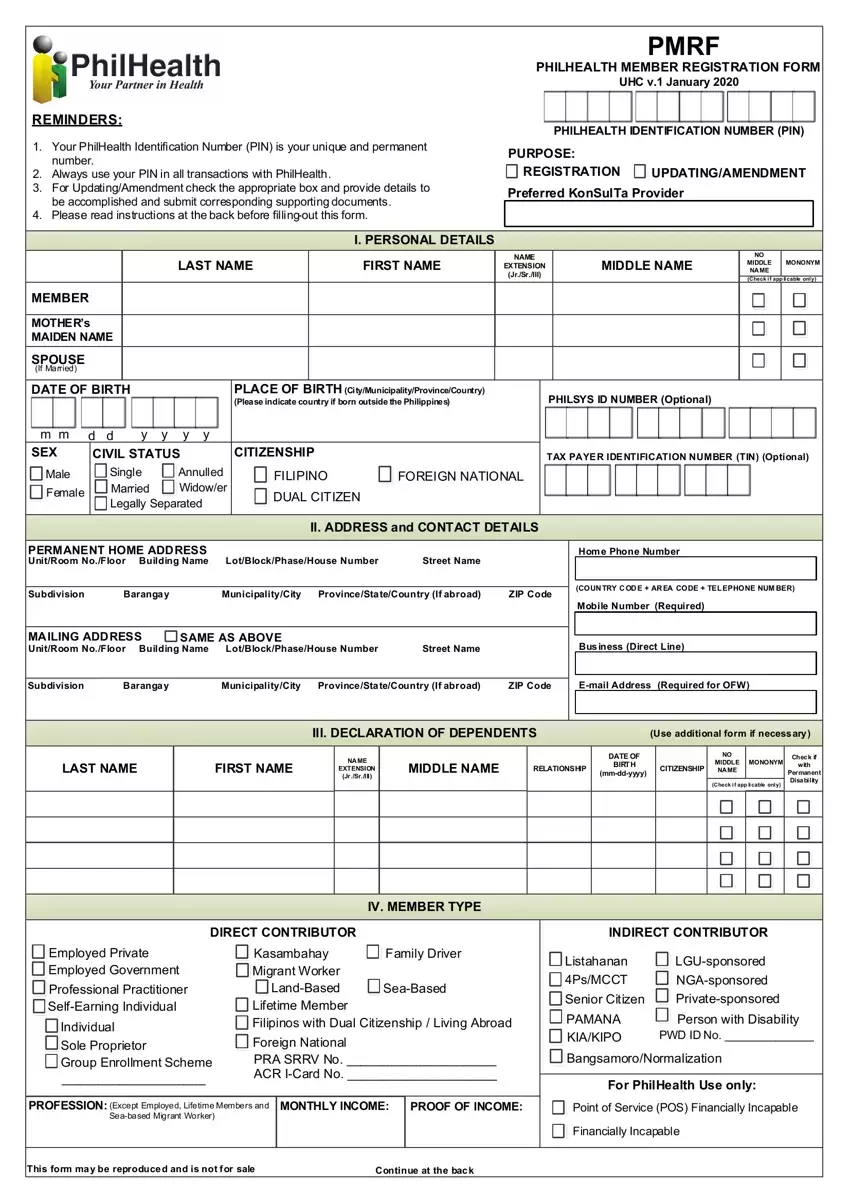
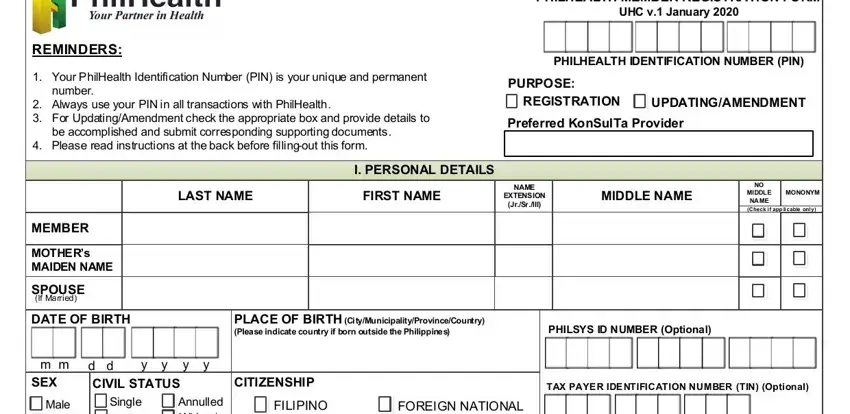
Change of Civil StatusWe chose the top programmers to create our PDF editor. This app will help you prepare the philhealth form form effortlessly and won't require too much of your energy. This simple procedure may help you learn how to start.
Step 1: Choose the "Get Form Now" button to start out.
Step 2: At this point, you can begin modifying the philhealth form. Our multifunctional toolbar is at your disposal - add, remove, adjust, highlight, and do similar commands with the content material in the document.
To get the document, provide the information the system will require you to for each of the next segments:
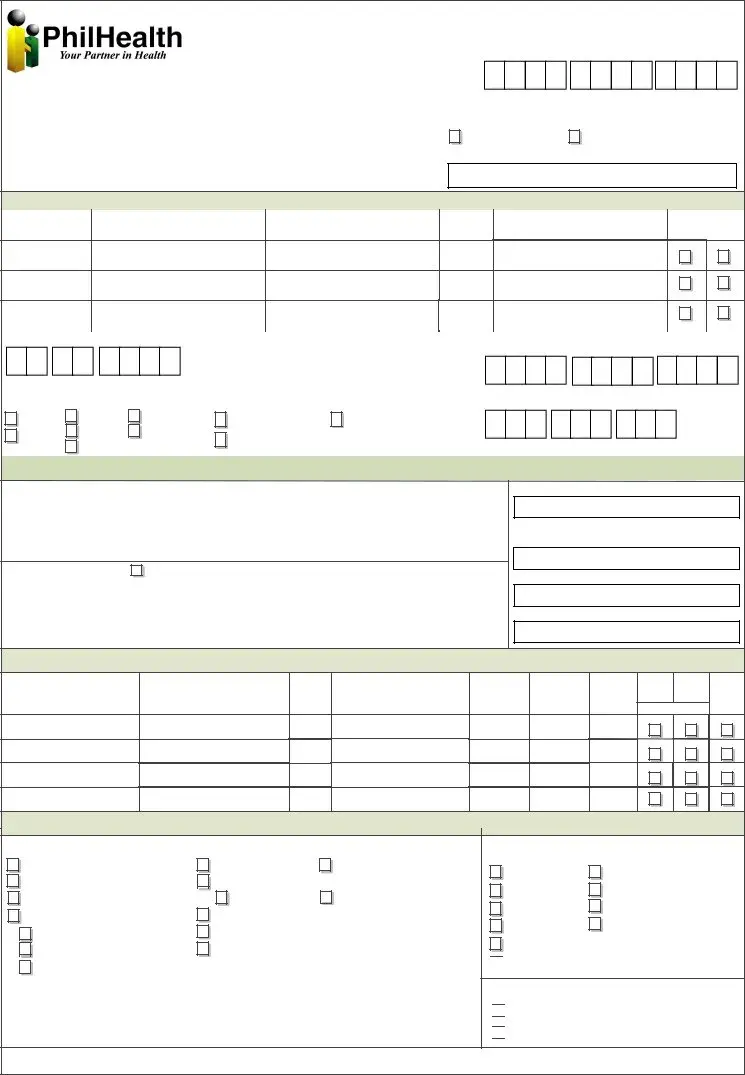
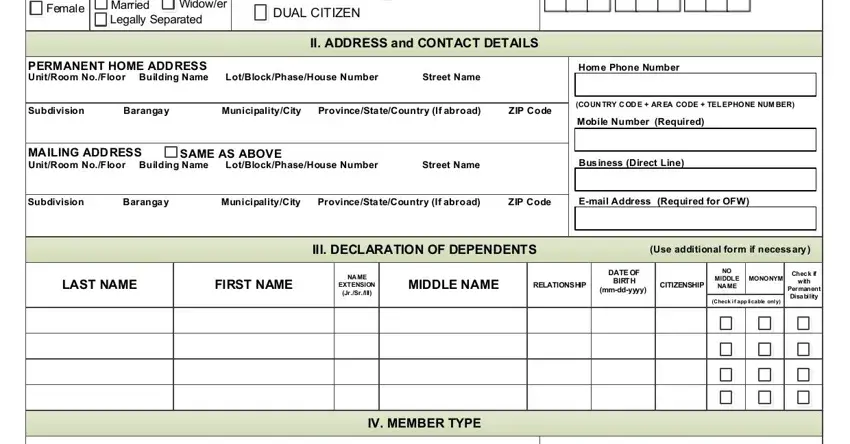
Type in the data in the Female, Single Married Legally Separated, Annulled Widower, DUAL CITIZEN, II ADDRESS and CONTACT DETAILS, PERMANENT HOME ADDRESS UnitRoom, Hom e Phone Number, Subdivision Baranga y, COUN TRY C OD E AR EA CODE TEL, Mobile Number Required, MAILING ADDRESS UnitRoom NoFloor, SAME AS ABOVE, Bus iness Direct Line, Subdivision Baranga y, and Email Address Required for OFW field.
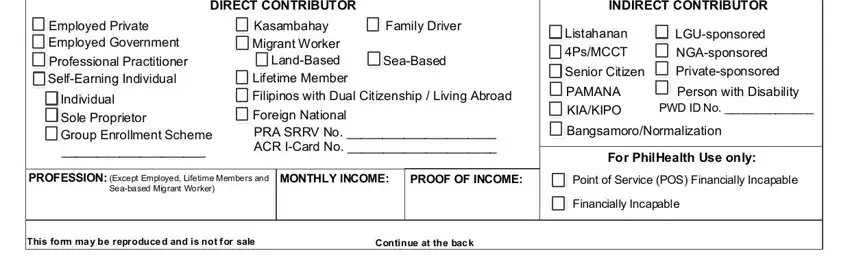
You should be requested for some relevant information to be able to fill in the DIRECT CONTRIBUTOR, INDIRECT CONTRIBUTOR, Employed Private Employed, Professional Practitioner, Individual Sole Proprietor Group, Kasambahay Family Driver Migrant, SeaBased, Foreign National PRA SRRV No ACR, Listahanan PsMCCT, Senior Citizen, PAMANA KIAKIPO, LGUsponsored NGAsponsored, Person with Disability PWD ID No, BangsamoroNormalization, and For PhilHealth Use only section.
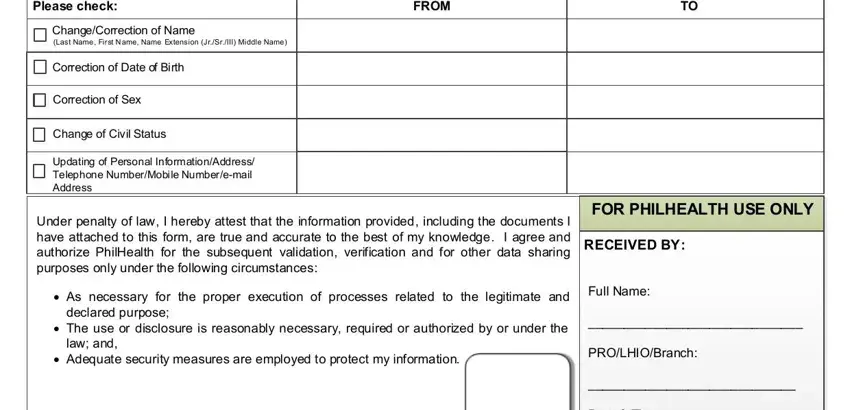
In the section Please check, FROM, ChangeCorrection of Name Last Name, Correction of Date of Birth, Correction of Sex, Change of Civil Status, Updating of Personal, Under penalty of law I hereby, FOR PHILHEALTH USE ONLY, RECEIVED BY, As necessary for the proper, Full Name, declared purpose, The use or disclosure is, and law and, include the rights and obligations of the parties.
Step 3: When you click on the Done button, your final document is simply exportable to all of your gadgets. Alternatively, you will be able to send it via mail.
Step 4: Make a copy of each form. It would save you time and assist you to avoid concerns as time goes on. Keep in mind, your details isn't going to be used or analyzed by us.
