

Making use of the online PDF tool by FormsPal, you are able to fill in or edit foot physical exam right here and now. Our editor is constantly developing to grant the best user experience attainable, and that's because of our resolve for constant development and listening closely to customer feedback. It merely requires several simple steps:
Step 1: Hit the "Get Form" button above. It'll open our tool so you can begin completing your form.
Step 2: The tool allows you to customize PDF documents in various ways. Transform it with any text, adjust original content, and put in a signature - all possible within a few minutes!
When it comes to blanks of this particular document, here's what you should know:
1. When completing the foot physical exam, ensure to complete all necessary blanks within its relevant part. This will help hasten the work, allowing for your details to be handled promptly and accurately.
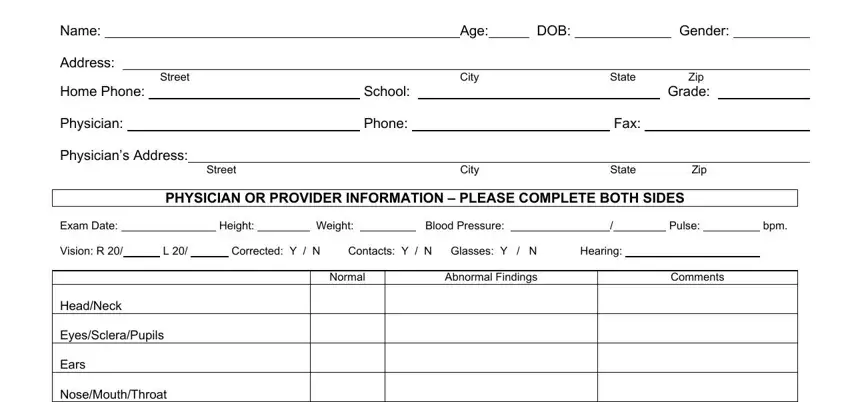
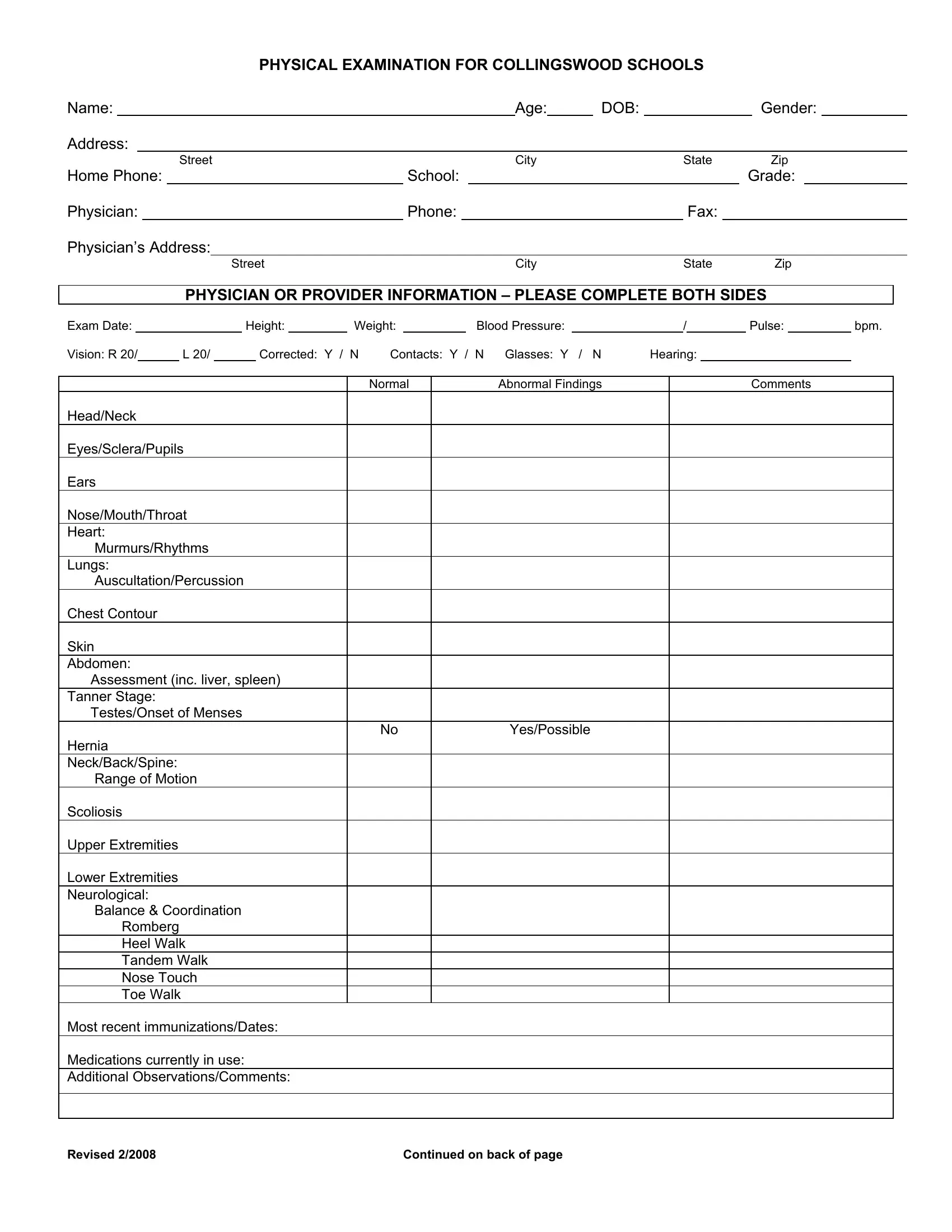
2. Once your current task is complete, take the next step – fill out all of these fields - Exam Date Vision R HeadNeck, and YesPossible with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
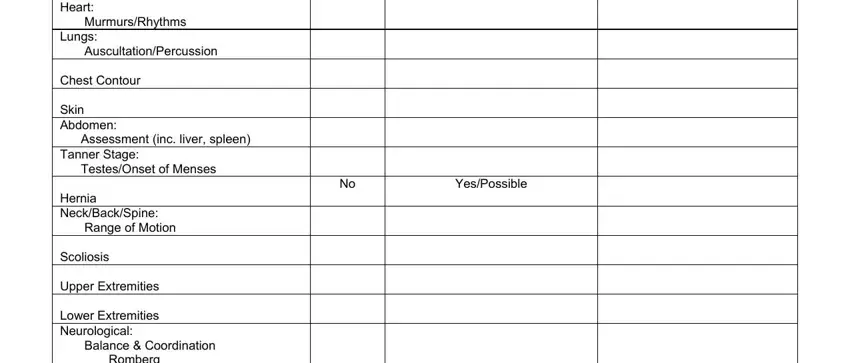
3. In this part, take a look at Exam Date Vision R HeadNeck, Revised, and Continued on back of page. Every one of these have to be completed with greatest focus on detail.
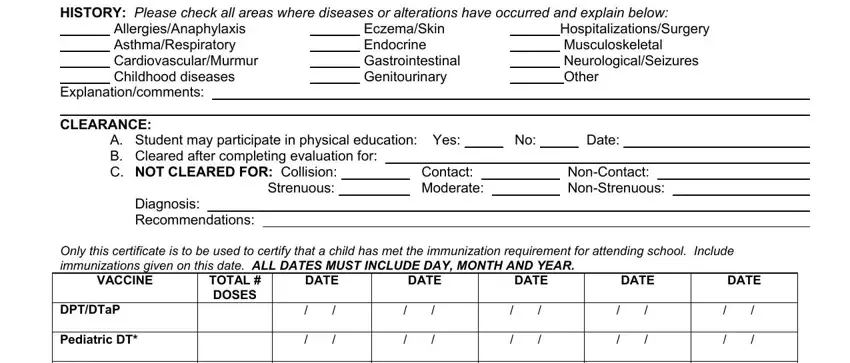
4. To move forward, the next stage involves completing several blank fields. These include HISTORY Please check all areas, AllergiesAnaphylaxis, EczemaSkin Endocrine, HospitalizationsSurgery, A Student may participate in, Contact Moderate, NonContact NonStrenuous, Only this certificate is to be, VACCINE, TOTAL DOSES, DATE, DATE, DATE, DATE, and DATE, which you'll find crucial to going forward with this particular PDF.
5. And finally, this final part is what you need to complete prior to using the document. The blanks here include the following: OPV, IPV, MMR, Measles, Mumps, Rubella, Hepatitis B, HIB or Prohibit, Varicella, Pneumococcal PCV, Meningococcal, RSV, and Influenza.
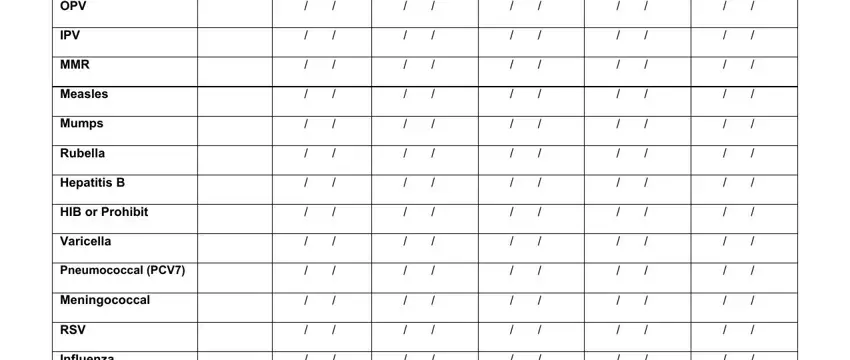
Be really careful when filling out Influenza and Pneumococcal PCV, since this is where a lot of people make some mistakes.
Step 3: Make sure that your details are right and just click "Done" to conclude the project. Try a free trial subscription at FormsPal and acquire immediate access to foot physical exam - with all adjustments preserved and accessible from your FormsPal account page. FormsPal provides secure document completion devoid of personal data recording or any type of sharing. Rest assured that your details are secure with us!