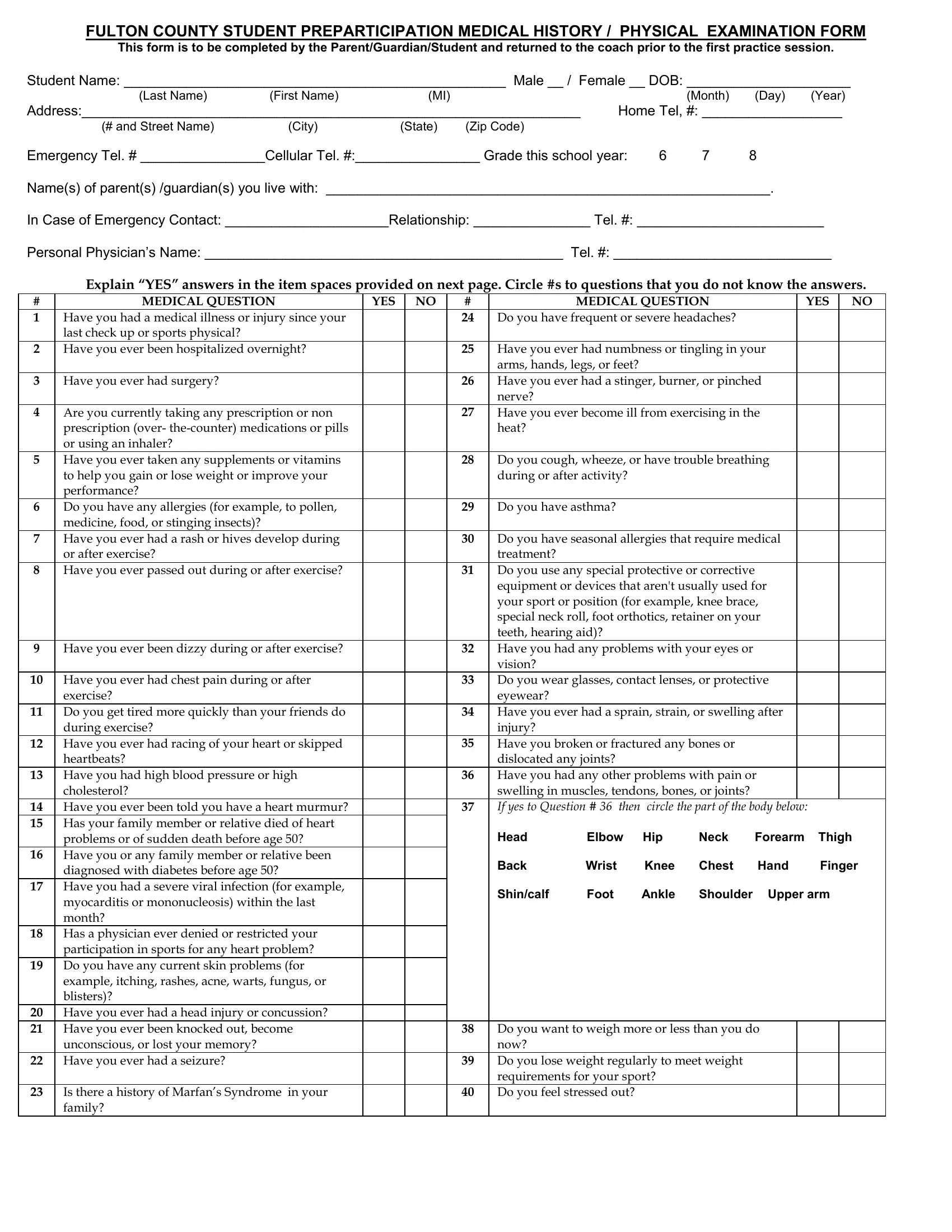
The Fulton County School Physical Form serves as a comprehensive document to ensure the safety and preparedness of students participating in athletic programs. Designed to be filled out by parents, guardians, or the students themselves, it collects detailed information on the student’s medical history, current health status, and physical readiness for participation in sports activities. The form initiates with personal details, such as the student's name, date of birth, contact information, and living situation. It then delves into a thorough medical history questionnaire that prompts responses to various health-related questions, ranging from illnesses, injuries, and hospitalizations to specifics about medications, allergies, and familial health history. The importance of accurately reporting past and present health conditions cannot be understated, as it ensures that coaches and medical personnel are well-informed of any risks or necessary precautions. Additionally, the form includes a section dedicated to the physical examination, conducted by a licensed physician, which assesses the student’s physical condition through various checks, including vision, heart rate, blood pressure, and musculoskeletal health. This meticulous health screening aims to identify any potential limitations or the need for special equipment that might influence a student’s ability to safely engage in athletic activities. Lastly, the form concludes with the physician’s clearance, indicating whether the student is medically approved to participate in interscholastic athletic practices and competitions, or if there are any restrictions or recommendations for further evaluation or rehabilitation. Overall, the Fulton County School Physical Form is a vital tool in promoting the health, safety, and well-being of student athletes, facilitating a thorough assessment to ensure they are physically and medically fit for participation in sports.
| Question | Answer |
|---|---|
| Form Name | Fulton County School Physical Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | mononucleosis, fulton county school medical forms, PREPARTICIPATION, L20 |