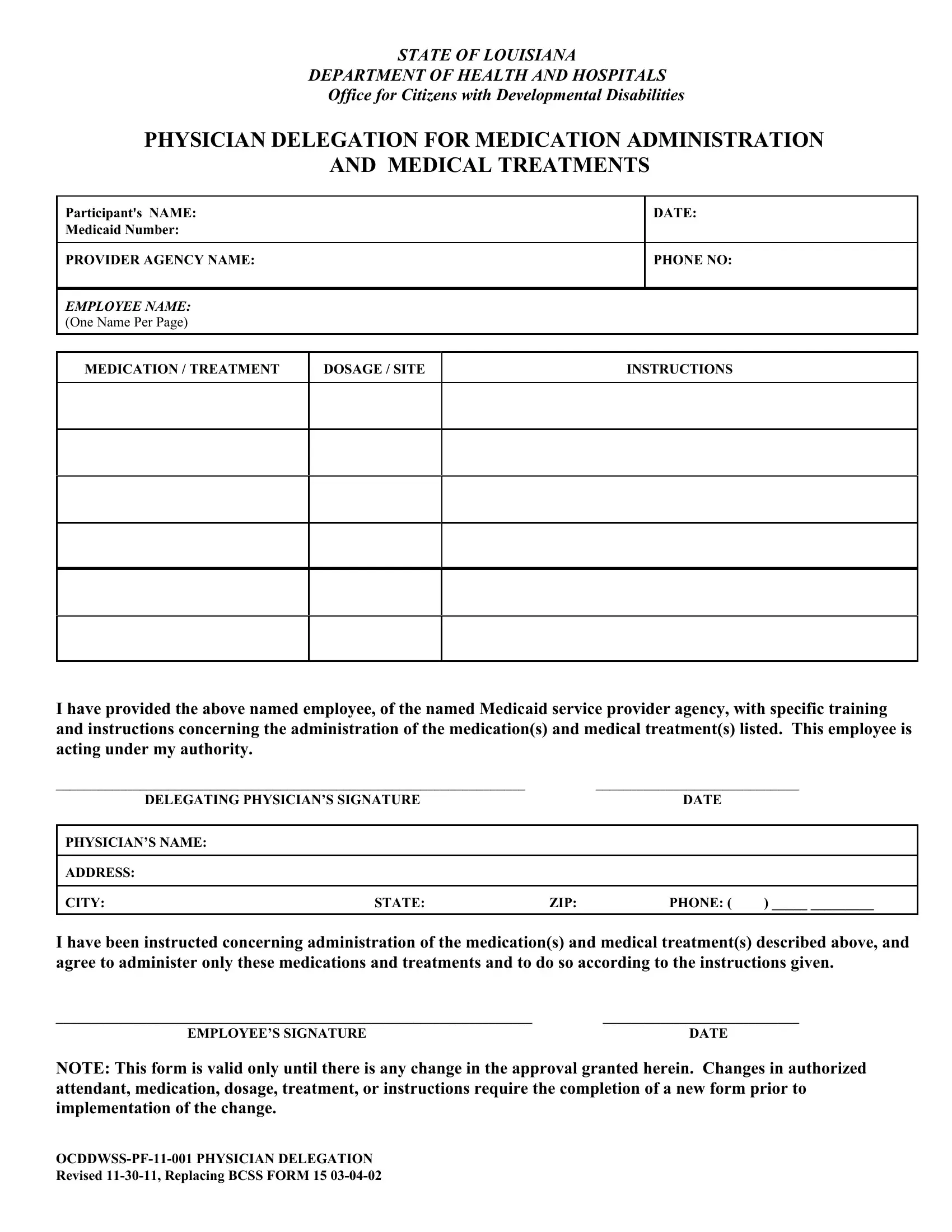
In the realm of healthcare and medicine, the dynamics of treatment extend beyond hospital rooms and into various settings where constant medical oversight is not always feasible. The Physician Delegation Form, as issued by the State of Louisiana's Department of Health and Hospitals, Office for Citizens with Developmental Disabilities, bridges this gap by authorizing non-physician personnel to administer medication and carry out medical treatments under a physician's supervision. This document not only specifies the participant's name and Medicaid number but also names the provider agency and its employee designated to perform these tasks. It meticulously outlines the type, dosage, and site of medication or treatment, ensuring that delegated individuals are directly instructed by the delegating physician. With spaces for both the physician's and the employee's signatures, it underscores a mutual agreement and understanding of the responsibilities handed over. Significantly, this form is contingent on the precision of its contents—any change in treatment, medication, or personnel necessitates a new form, emphasizing the form's pivotal role in safeguarding patient care through clear, regulated delegation.
| Question | Answer |
|---|---|
| Form Name | Physician Delegation Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | ocddwss pf 11 001 physician delegation, nurse delegation form for colostomy louisiana, louisiana physician delegation, louisiana delegation administration |
STATE OF LOUISIANA
DEPARTMENT OF HEALTH AND HOSPITALS
Office for Citizens with Developmental Disabilities
PHYSICIAN DELEGATION FOR MEDICATION ADMINISTRATION
AND MEDICAL TREATMENTS
Participant's NAME:
Medicaid Number:
PROVIDER AGENCY NAME:
EMPLOYEE NAME: (ONE NAME PER PAGE)
DATE:
PHONE NO:
MEDICATION / TREATMENT
DOSAGE / SITE
INSTRUCTIONS
I have provided the above named employee, of the named Medicaid service provider agency, with specific training and instructions concerning the administration of the medication(s) and medical treatment(s) listed. This employee is acting under my authority.
___________________________________________________________________ |
|
_____________________________ |
||
DELEGATING PHYSICIAN’S SIGNATURE |
|
DATE |
|
|
|
|
|
|
|
PHYSICIAN’S NAME: |
|
|
|
|
|
|
|
|
|
ADDRESS: |
|
|
|
|
|
|
|
|
|
CITY: |
STATE: |
ZIP: |
PHONE: ( |
) _____ _________ |
|
|
|
|
|
I have been instructed concerning administration of the medication(s) and medical treatment(s) described above, and agree to administer only these medications and treatments and to do so according to the instructions given.
____________________________________________________________________ |
____________________________ |
EMPLOYEE’S SIGNATURE |
DATE |
NOTE: This form is valid only until there is any change in the approval granted herein. Changes in authorized attendant, medication, dosage, treatment, or instructions require the completion of a new form prior to implementation of the change.
Revised