
FormsPal makes it easy to fill out the California Participating Practitioner Form online. Our PDF editor is free to use and continuously updated based on user feedback. Follow the steps below to complete your form:
Step 1: Click the "Get Form" button at the top of this page to open the PDF editor.
Step 2: Once the editor loads, you can fill in all required fields, add text, insert a signature, and make other changes to the document.
When completing the form, provide accurate information in every blank:
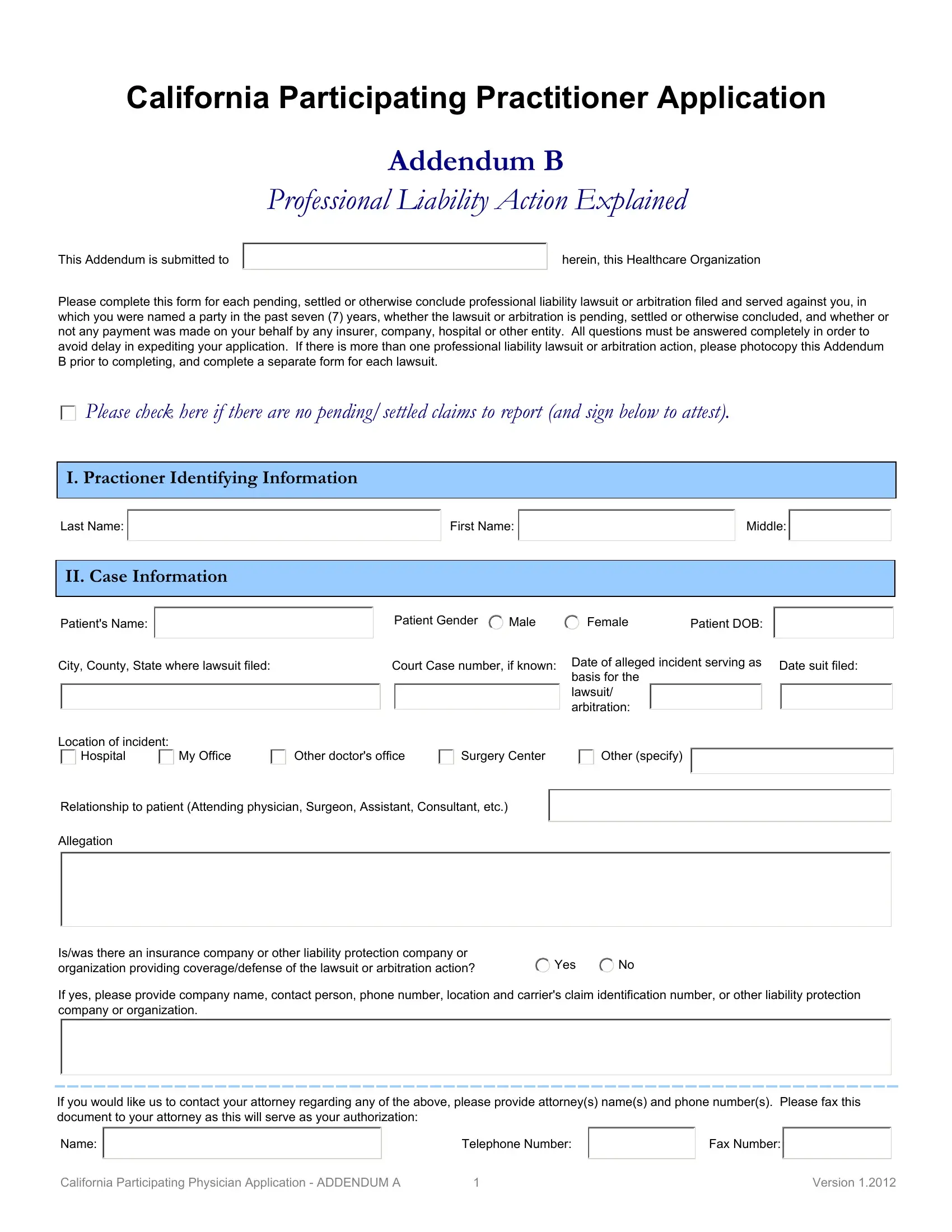
1. Begin with your identification details at the top of the form. Fill in your name, license number, specialty, and other required personal information:
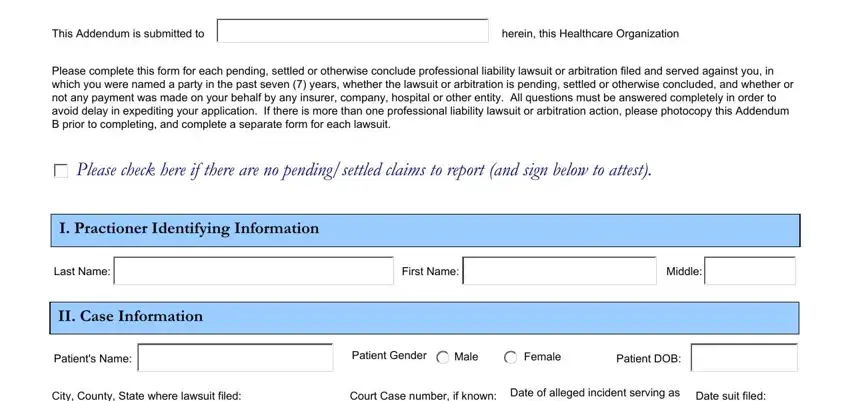
2. For each liability case, complete the case details: city, county, and state where the lawsuit was filed, court case number, date of the incident, date the suit was filed, location of the incident, and your relationship to the patient. Also fill in the allegation description and insurance information:
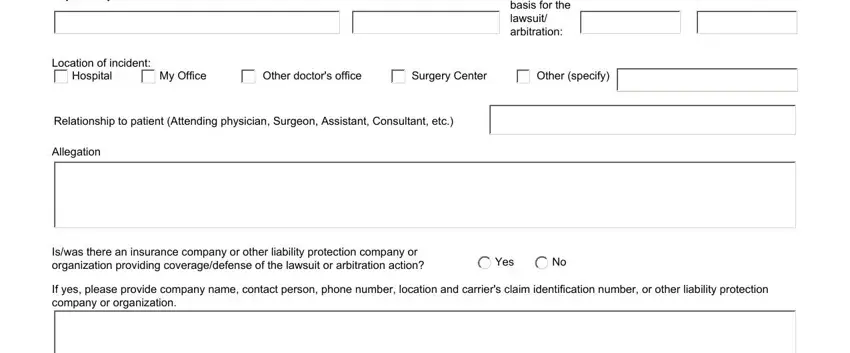
Double-check the Allegation field carefully before moving to the next section.
3. Complete the contact section with your telephone number, fax number, and any remaining identification fields:

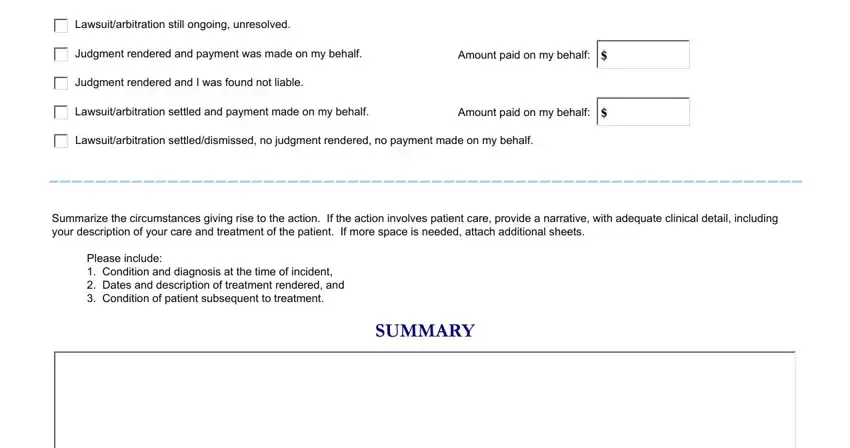
4. For each case, complete the outcome section: indicate whether the lawsuit is still ongoing, any judgment rendered, amounts paid on your behalf, and a written summary covering the circumstances and patient condition:
Step 3: After reviewing all entries, click "Done" to save your completed form. Register for a free 7-day trial to access and download your document at any time. FormsPal uses a secure system that never stores or shares your personal information.
Common Questions About the California Participating Practitioner Form
Who must complete this form? Medical practitioners applying to join California healthcare organizations must complete this form to disclose professional liability history from the past seven years.
What time period does the form cover? The form requires disclosure of all pending, settled, or concluded lawsuits or arbitration actions from the past seven years, regardless of outcome.
Can I fill it out online? Yes. FormsPal provides a free online PDF editor that lets you complete the California Participating Practitioner Application directly in your browser and download the finished document.
For related credentialing forms, see the Credentialing Application, the Participating Physician Application, and the Health Practitioner Physical Assessment Form.