
Using PDF forms online is certainly a breeze with this PDF tool. Anyone can fill in missouri handicap placard physician form here effortlessly. To retain our tool on the forefront of practicality, we strive to put into practice user-driven features and improvements on a regular basis. We are always happy to get suggestions - join us in reshaping how we work with PDF files. If you are seeking to begin, here's what it will take:
Step 1: Access the PDF file in our tool by clicking the "Get Form Button" above on this webpage.
Step 2: As soon as you launch the editor, you will find the document ready to be filled out. Aside from filling out different fields, you could also perform various other things with the file, namely writing your own textual content, changing the initial text, adding illustrations or photos, affixing your signature to the form, and more.
With regards to the blanks of this particular document, here's what you want to do:
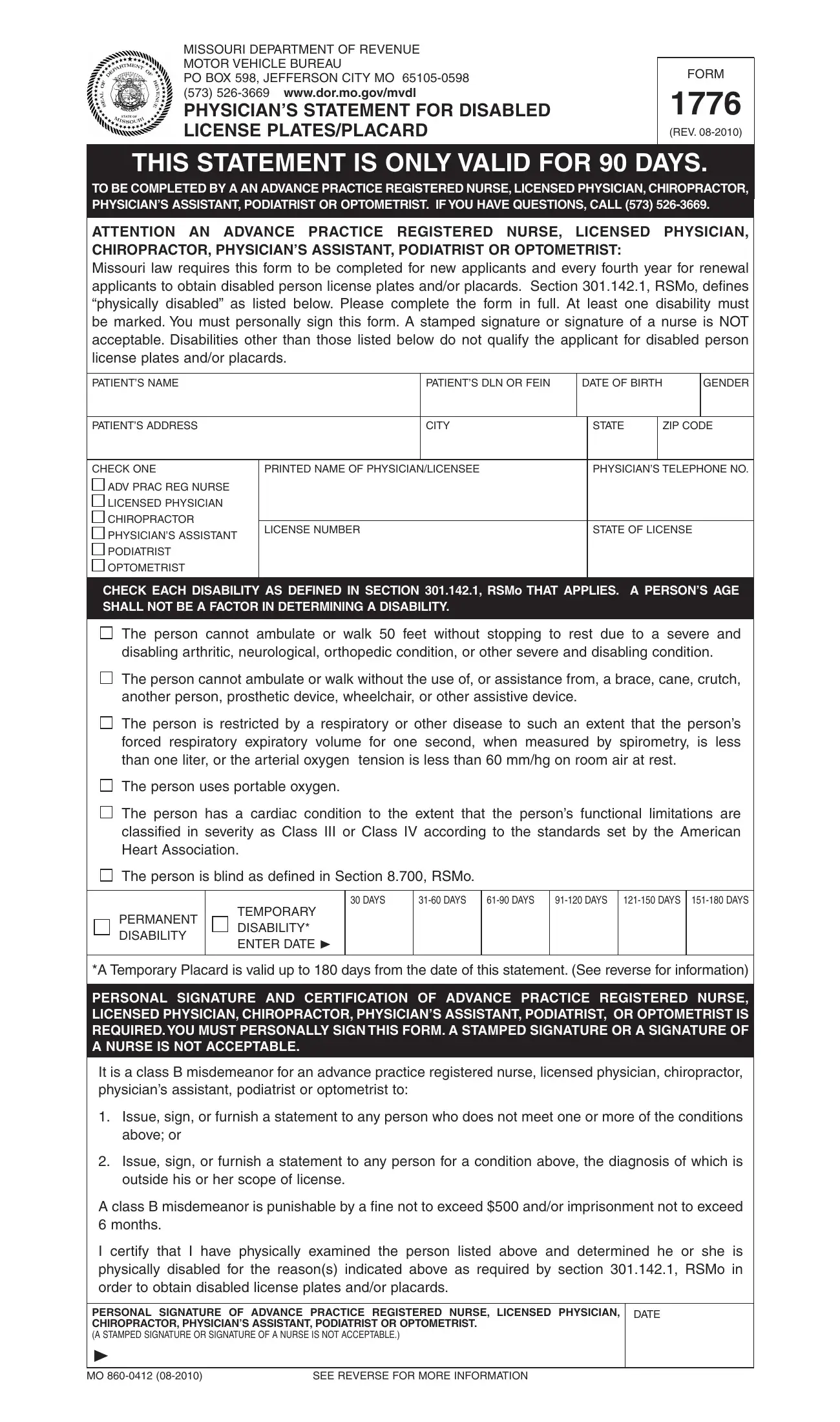
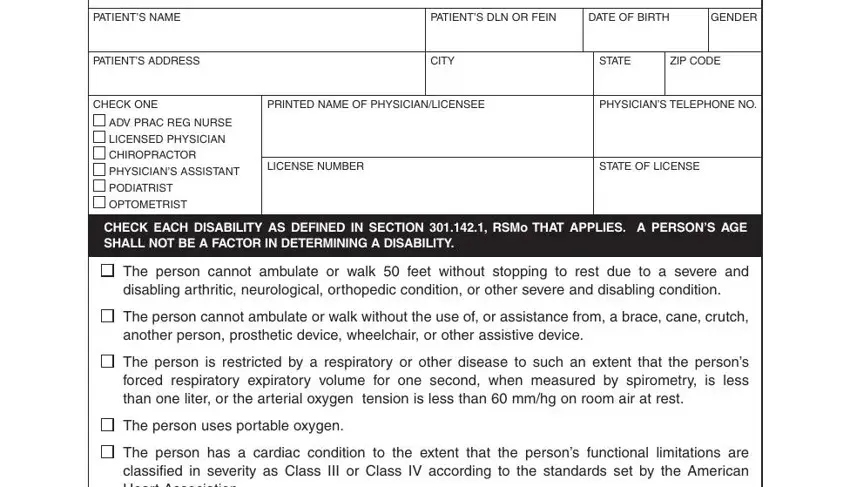
1. Begin filling out the missouri handicap placard physician form with a group of essential fields. Gather all of the important information and ensure not a single thing forgotten!
2. Once your current task is complete, take the next step – fill out all of these fields - The person has a cardiac condition, The person is blind as defined in, DAYS, DAYS, DAYS, DAYS, DAYS DAYS, PERMANENT DISABILITY, TEMPORARY DISABILITY ENTER DATE, A Temporary Placard is valid up to, PERSONAL SIGNATURE AND, It is a class B misdemeanor for an, Issue sign or furnish a statement, Issue sign or furnish a statement, and A class B misdemeanor is with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
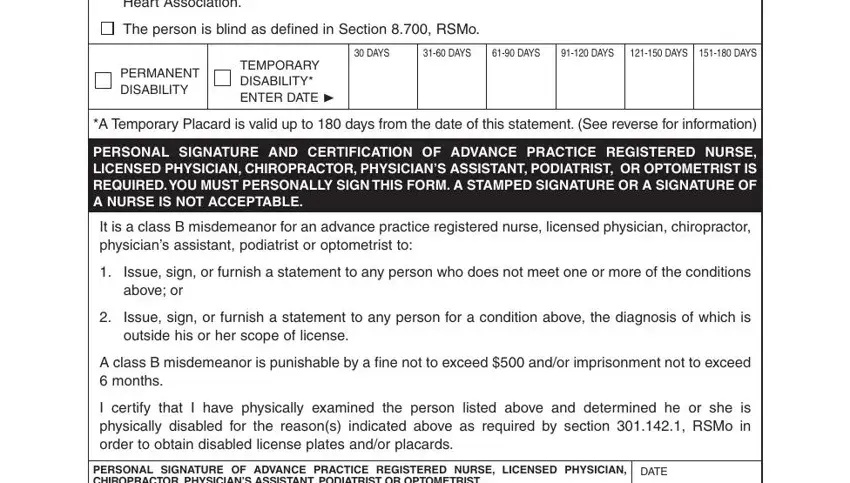
3. This next portion is related to PERSONAL SIGNATURE OF ADVANCE, and SEE REVERSE FOR MORE INFORMATION - fill out every one of these blanks.

Be very attentive when completing SEE REVERSE FOR MORE INFORMATION and SEE REVERSE FOR MORE INFORMATION, as this is the section where many people make some mistakes.
Step 3: Go through the information you've inserted in the form fields and then hit the "Done" button. Join FormsPal now and instantly use missouri handicap placard physician form, all set for downloading. All alterations you make are kept , allowing you to edit the file at a later point anytime. With FormsPal, you can certainly fill out documents without stressing about personal information breaches or records getting distributed. Our protected software ensures that your private data is kept safe.