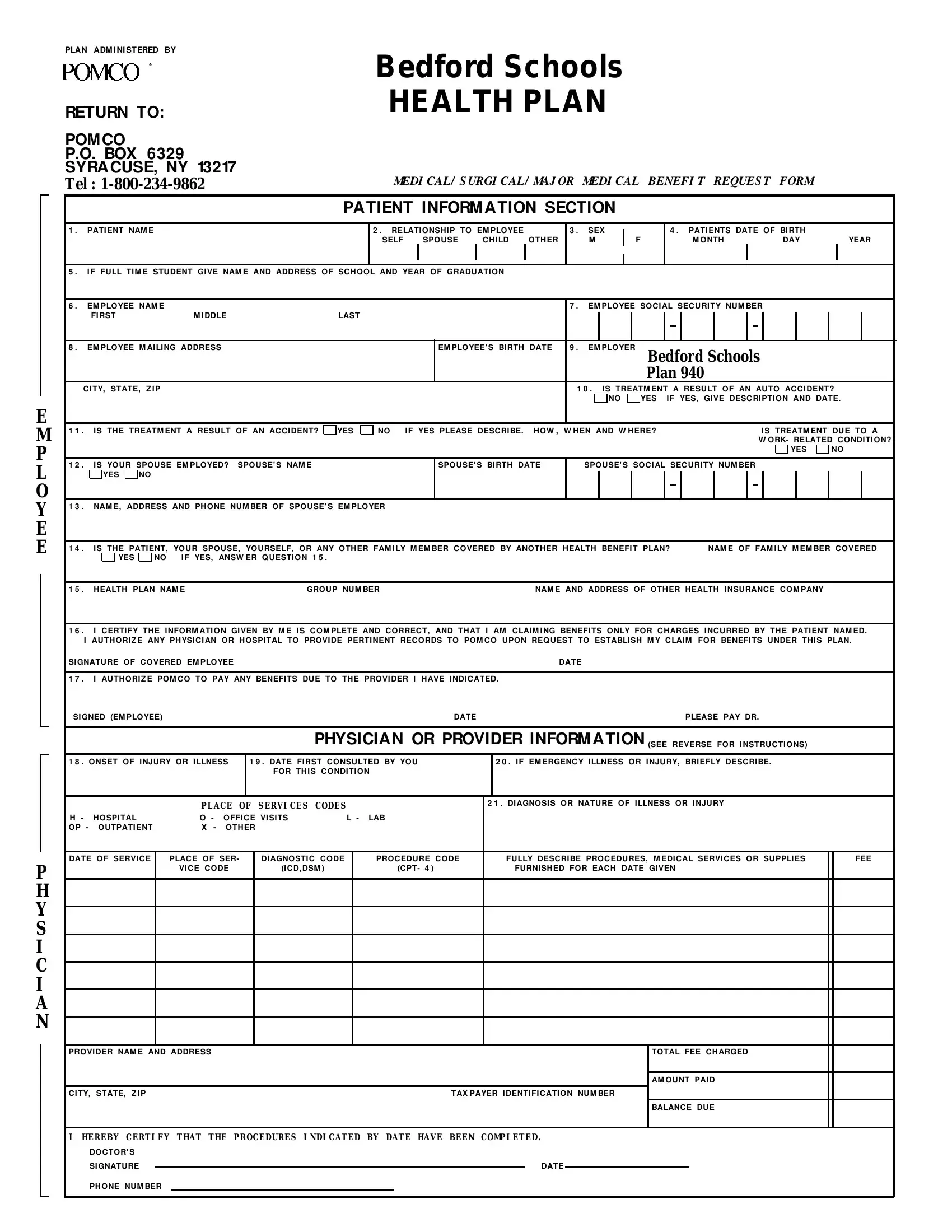
Navigating through healthcare forms can sometimes feel like deciphering an ancient script. The Pomco form is a crucial document for employees covered under Bedford Schools' health plan, simplifying the process of submitting medical, surgical, or major medical benefit requests. Located in Syracuse, NY, the form is designed to streamline communication between patients, healthcare providers, and the insurer. It covers essential patient information, including personal details, employment, and the nature of the treatment or injury. Notably, the form addresses cases where treatment results from accidents, whether auto-related or otherwise, and determines if the treatment is for a work-related condition. It also inquires about any other health benefit plans that may cover the patient, laying the groundwork for coordination of benefits. By requiring signatures to authorize information sharing and payment to healthcare providers, the form upholds transparency and consent. Instructions on the reverse side aim to minimize errors and delays by guiding patients on how to correctly fill out the form, including a reminder of the potential legal repercussions of submitting false information. This comprehensive approach ensures that claims are processed efficiently, benefiting both the claimants and the administrators of the health plan.
| Question | Answer |
|---|---|
| Form Name | Pomco Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | medical form pomco ny, pomco claims address, pomco prior authorization form, pomco select firmagon authoriation forms |
E
M
P
L
O Y E E
P H Y S I C I A N
PLAN |
ADM I NI STERED BY |
|
|
|
|
|
|
|
Bedford Schools |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
RETURN TO: |
|
|
|
|
|
|
|
|
HEALTH PLAN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
POM CO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
P.O. BOX |
6329 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
SYRA CUSE, NY 13217 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Tel : |
|
|
|
|
|
|
|
|
MEDI CAL/ S URGI CAL/ MAJ OR MEDI CAL BENEFI T REQUES T |
FORM |
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
PA TIENT INFORM A TION SECTION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
1 . |
PATI ENT NAM E |
|
|
|
|
|
|
|
|
2 . |
RELATI ONSH I P TO EM PLOYEE |
|
3 . |
SEX |
|
|
4 . |
PATI ENTS DATE OF BI RTH |
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
SELF SPOU SE |
C H I LD |
OTH ER |
|
M |
|
F |
|
|
|
M ONTH |
DAY |
YEAR |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
5 . I F FU LL TI M E STU DENT GI VE NAM E AND ADDRESS OF SC H OOL AND YEAR OF GRADU ATI ON |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
6 . |
EM PLOYEE NAM E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7 . |
EM PLOYEE SOC I AL SEC U RI TY NU M BER |
|
|
|
|
|
||||||||||||||
|
FI RST |
|
|
M I DDLE |
|
|
|
LAST |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 . |
EM PLOYEE M AI LI NG ADDRESS |
|
|
|
|
|
|
|
EM PLOYEE' S BI RTH DATE |
9 . |
EM PLOYER |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Bedford Schools |
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Plan 940 |
|
|
|
|
|
|||||||||
C I TY, STATE, |
Z I P |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 0 . I S TREATM ENT A RESU LT OF AN AU TO AC C I DENT? |
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NO |
|
YES I F YES, GI VE DESC RI PTI ON AND DATE. |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
1 1 . |
I S TH E TREATM ENT A RESU LT OF AN AC C I DENT? |
YES |
NO |
I F YES PLEASE DESC RI BE. |
H OW , W H EN AND W H ERE? |
|
|
|
|
I S TREATM ENT DU E TO A |
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
W ORK- RELATED C ONDI TI ON? |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
NO |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
1 2 . |
I S YOU R SPOU SE EM PLOYED? SPOU SE' S NAM E |
|
|
|
|
SPOU SE' S BI RTH DATE |
|
SPOU SE' S SOC I AL SEC U RI TY NU M BER |
|
|
|
|
|
|||||||||||||||||||||||
|
YES NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 3 . |
NAM E, ADDRESS AND PH ONE NU M BER OF SPOU SE' S EM PLOYER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|||||||||||||||||||||||||||||||||
1 4 . |
I S TH E PATI ENT, YOU R SPOU SE, YOU RSELF, OR ANY OTH ER FAM I LY M EM BER C OVERED BY ANOTH ER H EALTH BENEFI T PLAN? |
NAM E OF FAM I LY M EM BER C OVERED |
|
|||||||||||||||||||||||||||||||||
|
YES |
NO |
I F YES, |
ANSW ER Q U ESTI ON 1 5 . |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
1 5 . |
H EALTH PLAN NAM E |
|
|
|
|
GROU P NU M BER |
|
|
|
|
NAM E AND ADDRESS OF OTH ER H EALTH I NSU RANC E C OM PANY |
|
|
|
||||||||||||||||||||||
|
|
|
||||||||||||||||||||||||||||||||||
1 6 . |
I C ERTI FY TH E I NFORM ATI ON GI VEN BY M E I S C OM PLETE AND C ORREC T, AND TH AT I AM C LAI M I NG BENEFI TS ONLY FOR C H ARGES I NC U RRED BY TH E PATI ENT NAM ED. |
|
||||||||||||||||||||||||||||||||||
I AU TH ORI Z E ANY PH YSI C I AN OR H OSPI TAL TO PROVI DE PERTI NENT REC ORDS TO POM C O U PON REQ U EST TO ESTABLI SH M Y C LAI M FOR BENEFI TS U NDER TH I S PLAN. |
|
|||||||||||||||||||||||||||||||||||
SI GNATU RE OF C OVERED EM PLOYEE |
|
|
|
|
|
|
|
|
|
|
DATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
1 7 . |
I AU TH ORI Z E POM C O TO PAY ANY BENEFI TS DU E TO TH E PROVI DER I H AVE I NDI C ATED. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
SI GNED (EM PLOYEE) |
|
|
|
|
|
|
|
|
|
|
DATE |
|
|
|
|
|
|
|
|
|
|
|
PLEASE PAY DR. |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
PHYSICIA N OR PROVIDER INFORM A TION (SEE REVERSE FOR I NSTRU C TI ONS) |
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
1 8 . ONSET OF I NJU RY OR I LLNESS |
|
1 9 . DATE FI RST C ONSU LTED BY YOU |
|
2 0 . I F EM ERGENC Y I LLNESS OR I NJU RY, |
BRI EFLY DESC RI BE. |
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
FOR TH I S C ONDI TI ON |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
PLACE |
OF S ERVI CES CODES |
|
|
|
2 1 . DI AGNOSI S OR NATU RE OF I LLNESS OR I NJU RY |
|
|
|
|
|
||||||||||||||||||||||
H - |
H OSPI TAL |
|
|
O |
- |
OFFI C E VI SI TS |
L - |
LAB |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
OP - OU TPATI ENT |
X |
- |
OTH ER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
DATE OF SERVI C E |
|
PLAC E OF SER- |
|
|
DI AGNOSTI C C ODE |
|
PROC EDU RE C ODE |
|
FU LLY DESC RI BE PROC EDU RES, M EDI C AL SERVI C ES OR SU PPLI ES |
FEE |
|
|||||||||||||||||||||||||
|
|
|
|
VI C E C ODE |
|
|
(I C D, DSM ) |
|
|
|
(C PT- 4 ) |
|
FU RNI SH ED FOR EAC H |
DATE GI VEN |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PROVI DER NAM E AND ADDRESS |
|
|
TOTAL FEE C H ARGED |
|
|
|
|
|
|
|
AM OU NT PAI D |
C I TY, STATE, Z I P |
TAX PAYER I DENTI FI C ATI ON NU M BER |
||
|
|
|
BALANC E DU E |
I HEREBY CERTI FY THAT THE PROCEDURES |
I NDI CATED BY DATE HAVE BEEN COMPLETED. |
||||
DOC TOR' S |
|
|
|
||
SI GNATU RE |
|
|
|
DATE |
|
|
|
|
|||
PH ONE NU M BER |
|
|
|
|
|

Bedford Schools
HEALTH PLAN
HOW TO REQUEST BENEFITS
1 . COM PLETE ITEM S 1 THROUGH 1 0 UNDER THE PATIENT INFORM ATION SECTION. IF YOU ARE M ARRIED, OR HAVE OTHER HEALTH BENEFITS, ITEM S 1 2 ,1 3 ,1 4 , AND 1 5 M UST BE COM PLETED. IF ANY INFORM ATION IS M ISSING, IT WILL DELAY THE PAYM ENT OF YOUR CLAIM .
2 . HAVE YOUR DOCTOR COM PLETE THE PHYSICIAN'S INFORM ATION SECTION, OR SUBM IT COM PLETELY ITEM IZED BILLS. AN ITEM IZED BILL M UST CONTAIN: PATIENT'S NAM E, RELATIONSHIP, DATE OF SERVICE, TYPE OF SERVICE RENDERED, NATURE OF CONDITION BEING TREATED. IF THIS INFORM ATION IS M ISSING, YOU M AY WRITE IT ON THE BILL, AND SIGN YOUR NAM E. IF YOU GO TO A NON- PARTICIPATING PHARM ACY OR DO NOT USE YOUR PRE- SCRIPTION DRUG CARD, COM PLETE A SEPARATE PRESCRIPTION DRUG CLAIM FORM .
3 . IF YOU WANT BENEFITS PAID TO YOUR DOCTOR, OR PROVIDER DIRECTLY, BE SURE TO SIGN ITEM 1 7 .
4 . COM PLETE A SEPARATE CLAIM FORM FOR EACH FAM ILY M EM BER.
5 . THE COM PLETED CLAIM FORM SHOULD BE RETURNED TO:
POM CO
P.O. BOX 6329
SYRA CUSE, NY 13217
TOLL FREE NUMBER
IM PORTA NT REM INDER:
PLEA SE BE SURE THE EM PLOYEE'S SOCIA L SECURITY NUM BER HA S BEEN PROVIDED.
"ANY PERSON WHO KNOWINGLY AND WITH INTENT TO DEFRAUD FILES A STATEMENT OF CLAIM CONTAINING ANY MATERIALLY FALSE INFORMATION, OR CONCEALS FOR THE PURPOSE OF MISLEADING, INFORMATION CONCERNING ANY FACTUAL MATERIAL THERETO, COMMITS A FRAUDULENT INSURANCE ACT, WHICH IS A CRIME"