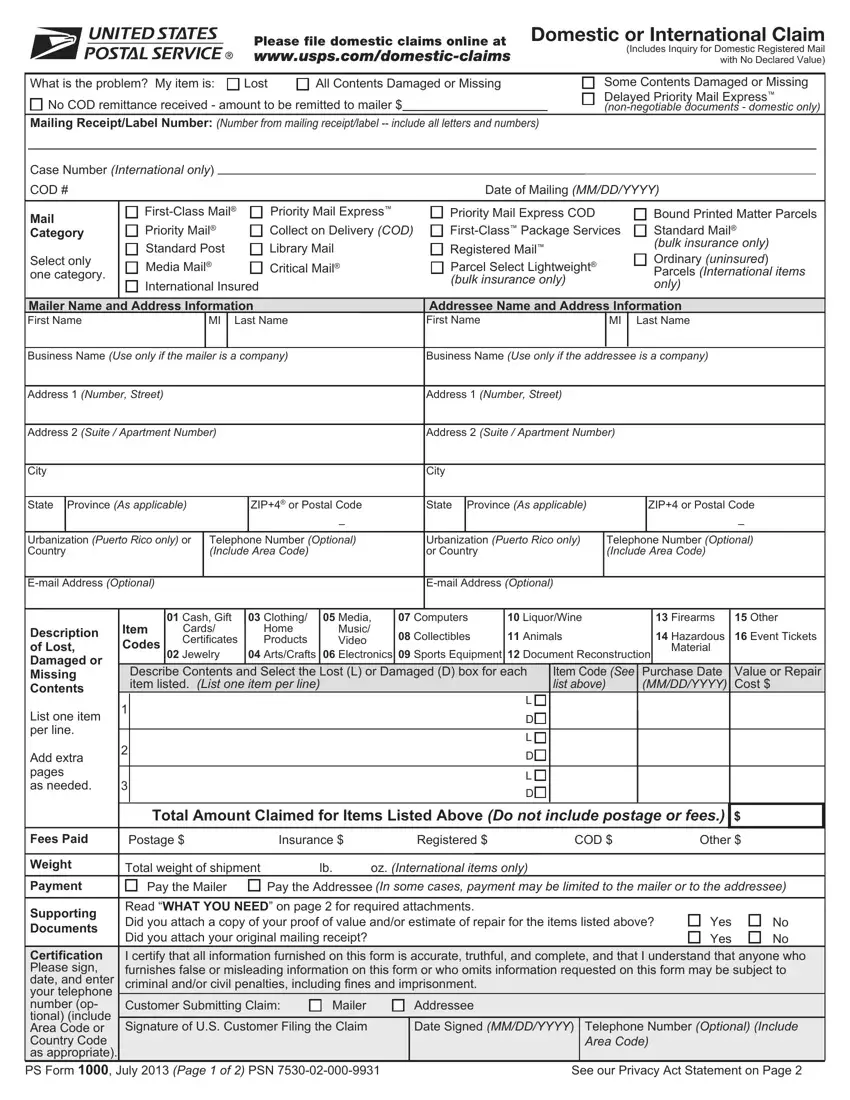
Domestic Claims:
Instructions – How to File a Domestic or International Claim or Inquiry for Domestic Registered Mail with No Declared Value
1.For faster service, please file your domestic claim online at www.usps.com/domestic-claims. If you are unable to file online, you may submit this form to: USPS Domestic Claims, PO Box 80143, St. Louis, MO 63180-0143.
2.Damaged/Missing Contents: Retain the mailing container, including wrapping, packaging, and any contents that were received, and upon written request, you must make them available to the local Post Office™ for inspection, retention, and disposition in accordance with the claims decision.
3.For more information about domestic claims, go to our Web site at www.usps.com/domestic-claims. Please retain copies of all documents mailed to St. Louis.
Domestic Registered Mail™ with No Declared Value Inquiry: Please complete this form and take it to your local Post Office™ for processing.
International Claims:
1.You must initiate an inquiry before filing a claim unless you are in the possession of a mailing with damaged or missing contents. You may initiate an inquiry by calling our International Inquiry Center at 1-800-222-1811.
2.If you are in possession of a mailing with damaged or missing contents (except an item from Canada), complete this form and present it and the damaged item(s), container, wrapping, packaging and any other contents received to a Post Office immediately. They will assist you in completing the claim.
3.If you are in possession of a mailing with damaged or missing contents mailed in Canada, contact the Canadian sender and instruct them to file the claim.
4.International claims may be payable to the mailer only or only to the addressee (varies by country). For more information about international inquiries and claims, see the Mailing Standards of the United States Postal Service, International Mail Manual at http://pe.usps.com or go to our Web site at www.usps.com/international-claims.
WHAT YOU NEED:
1.Your original mailing receipt for Insured, COD, Registered Mail™, Priority Mail International®, or Priority Mail Express™ service must be retained until the claim is resolved. Commercial customers will need the electronic manifest or hard copy PS Form 3877. Please retain a copy for your records.
2.Proof of value, such as a sales receipt (if applicable), invoice or bill of sale, or statement of costs for reconstruction of Priority Mail Express service documents. For online transactions, a copy of the canceled check, money order, credit card billing statement and the itemized email receipt or a final and itemized transaction receipt. If paid through an Internet account, an itemized transaction sheet indicating the amount deducted and the details of the transaction, including names, date, item(s) description, etc. Proof of value may be provided by either the mailer or addressee. Please retain a copy for your records.
3.Claims for damaged or missing contents:
a.See respective Domestic Claims and International Claim sections above.
b.Attach an estimate of repair costs from a reputable dealer for items to be repaired.
NOTE: If you are the addressee, do not return or remail any damaged items.
Time Limits for Filing Claims and Inquiries
Important: Read this information about time limits before filing a claim or inquiry.
Damaged or Missing Contents is defined as any mailing that has been received but some or all of the contents are damaged or missing. A Lost Article is defined as any mailing that has not been received and has not been returned to the sender.
|
Damaged |
Domestic Services |
International Services |
|
or |
|
|
|
|
|
You should file all claims for damaged or missing contents immediately, but |
You must file all claims for damaged or missing |
|
Missing |
|
Contents |
you must file no later than 60 days from the date of mailing. |
contents immediately. |
|
|
|
|
Types of Service |
When to File (from mailing date) |
|
|
No Sooner Than |
No Later Than |
|
|
|
|
|
|
|
|
|
|
|
|
|
DOMESTIC SERVICES |
|
|
|
|
|
Insured Mail, includes Priority Mail® |
21 Days |
180 |
Days |
|
|
COD |
45 Days |
180 Days |
|
|
Registered Mail™ |
15 Days |
180 |
Days |
|
|
Registered Mail COD |
45 Days |
180 |
Days |
|
Lost |
Priority Mail Express™ |
7 Days |
90 |
Days |
|
Articles |
Priority Mail Express COD |
45 Days |
90 |
Days |
|
|
APO/FPO Insured First-Class Mail®, space available (SAM), or parcel airlift (PAL) |
45 Days |
1 Year |
|
|
APO/FPO Insured (Surface Mail) |
75 Days |
1 Year |
|
|
INTERNATIONAL SERVICES |
|
|
|
|
|
Global Express Guaranteed® |
3 Days1 |
30 |
Days |
|
|
Priority Mail Express International |
3 Days2 |
90 |
Days |
|
|
Priority Mail Express International with guarantee |
3 Days1 |
30 Days3 |
|
|
Registered Mail and Priority Mail® International parcels |
7 Days |
6 Months |
|
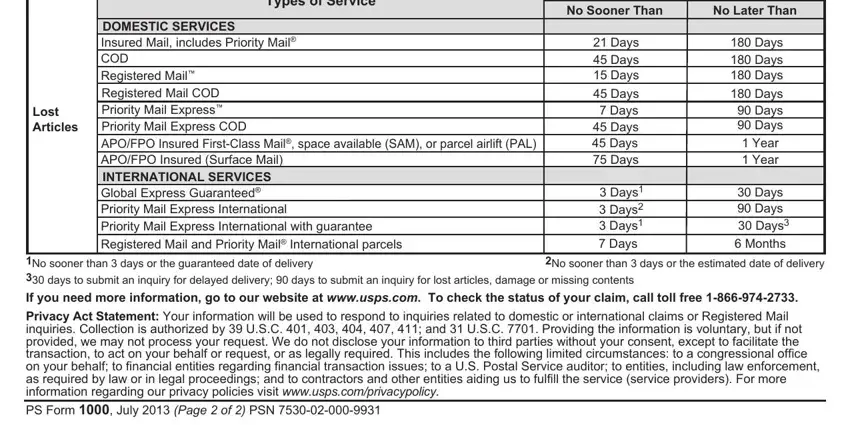
1No sooner than 3 days or the guaranteed date of delivery |
2No sooner than 3 days or the estimated date of delivery |
|
330 days to submit an inquiry for delayed delivery; 90 days to submit an inquiry for lost articles, damage or missing contents |
|
|
If you need more information, go to our website at www.usps.com. To check the status of your claim, call toll free 1-866-974-2733.
Privacy Act Statement: Your information will be used to respond to inquiries related to domestic or international claims or Registered Mail inquiries. Collection is authorized by 39 U.S.C. 401, 403, 404, 407, 411; and 31 U.S.C. 7701. Providing the information is voluntary, but if not provided, we may not process your request. We do not disclose your information to third parties without your consent, except to facilitate the transaction, to act on your behalf or request, or as legally required. This includes the following limited circumstances: to a congressional office on your behalf; to financial entities regarding financial transaction issues; to a U.S. Postal Service auditor; to entities, including law enforcement, as required by law or in legal proceedings; and to contractors and other entities aiding us to fulfill the service (service providers). For more information regarding our privacy policies visit www.usps.com/privacypolicy.
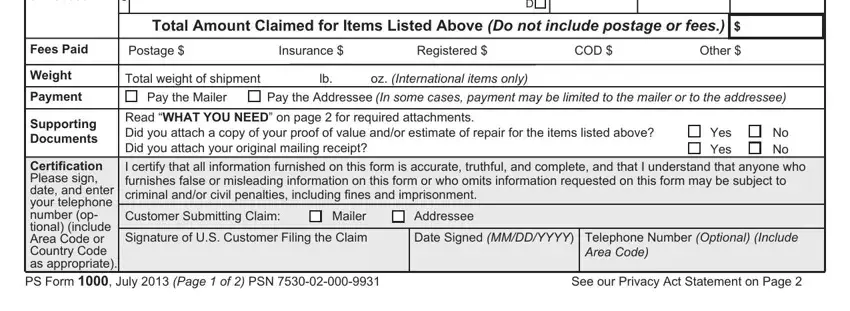
PS Form 1000, July 2013 (Page 2 of 2) PSN 7530-02-000-9931