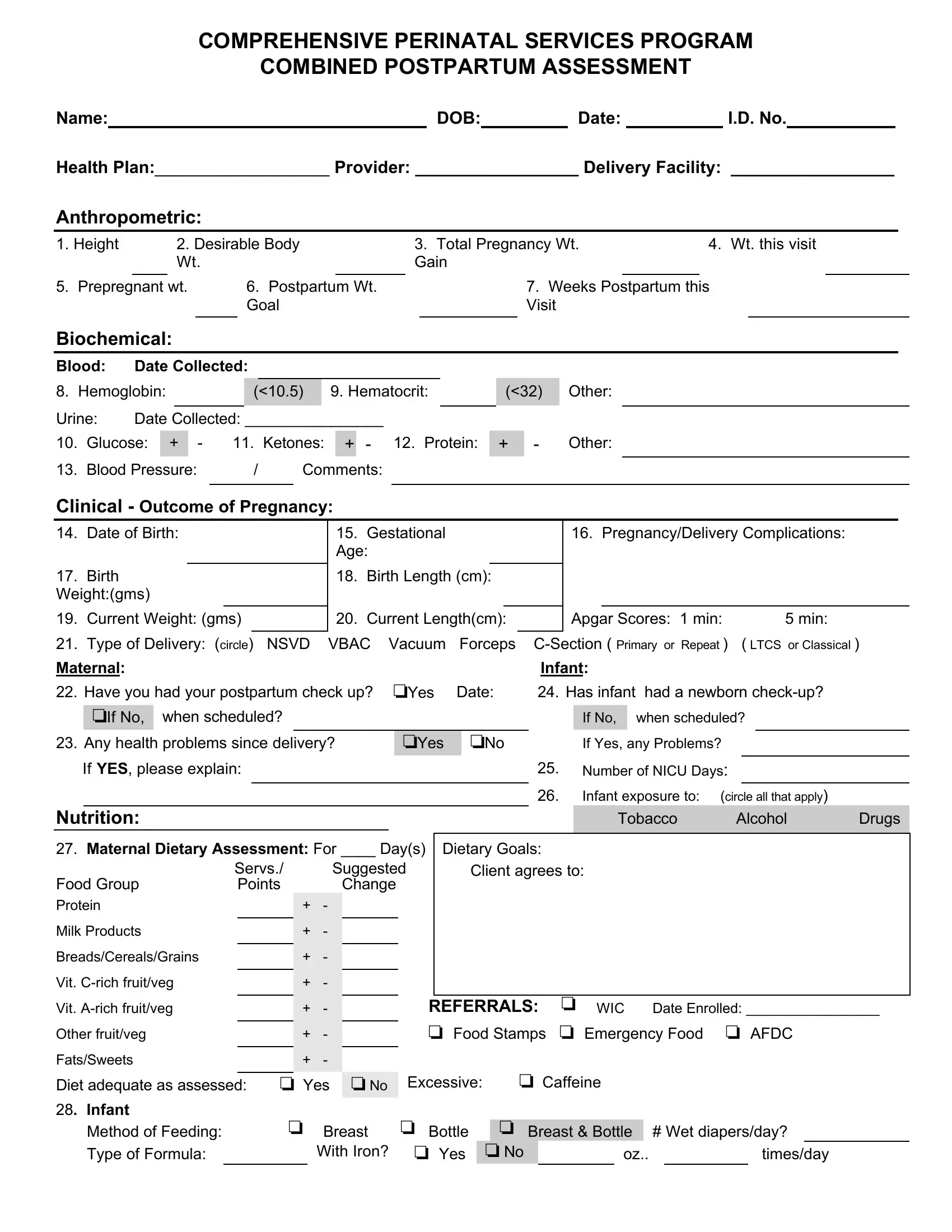
The Postpartum Assessment Example Form is a vital tool within the Comprehensive Perinatal Services Program, designed to guide healthcare providers in conducting thorough postpartum evaluations. This detailed form encompasses various elements crucial for assessing the well-being of both the mother and the newborn, subsequent to delivery. Key areas of assessment include anthropometric measurements, such as height, body weight goals, and postpartum weight, which offer insights into the physical recovery of the mother. Biochemical data, including hemoglobin and glucose levels, provide information on the mother's post-delivery health status. Furthermore, the form captures significant pregnancy and delivery details, including the outcome of the pregnancy, any complications, and the type of delivery, alongside the newborn's health metrics such as birth weight and current measurements. The form delves into maternal and infant nutrition, addressing dietary assessments and feeding methods, which are crucial for both mother and child's well-being. It also explores psychosocial aspects, inquiring about the mother’s emotional state, adjustments within the household, and the support system available for the new family. Additionally, healthcare referrals, educational needs, and a plan encompassing client goals and interventions are outlined. This comprehensive approach ensures that both the mother and the infant receive the care and support necessary during the critical postpartum period.
| Question | Answer |
|---|---|
| Form Name | Postpartum Assessment Example Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | postnatal assessment formates, postnatal assessment format, postnatal assessment format pdf, postpartum charting template |
COMPREHENSIVE PERINATAL SERVICES PROGRAM
COMBINED POSTPARTUM ASSESSMENT
Name:DOB: Date: I.D. No.
Health Plan:__________________ Provider: _________________ Delivery Facility: _________________
Anthropometric:
1. Height |
|
2. Desirable Body |
3. Total Pregnancy Wt. |
|
4. Wt. this visit |
|||||||
|
|
Wt. |
|
|
Gain |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
5. Prepregnant wt. |
6. Postpartum Wt. |
|
|
7. Weeks Postpartum this |
||||||||
|
|
|
|
Goal |
|
|
Visit |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Biochemical:
Blood: |
Date Collected: |
|
|
8. Hemoglobin: |
(<10.5) |
9. Hematocrit: |
|
Urine: |
Date Collected: ________________ |
10. |
Glucose: |
+ |
|
11. |
Ketones: |
+ |
12. |
Protein: |
13. |
Blood Pressure: |
|
/ |
Comments: |
|
|
||
(<32) Other:
+ Other:
Clinical Outcome of Pregnancy:
14. Date of Birth:
17.Birth
Weight:(gms)
19. Current Weight: (gms)
21. Type of Delivery: (circle) NSVD
15. |
Gestational |
|
16. Pregnancy/Delivery Complications: |
||||
Age: |
|
|
|
|
|||
|
|
|
|
|
|
|
|
18. |
Birth Length (cm): |
|
|
|
|
||
|
|
|
|
|
|
|
|
20. |
Current Length(cm): |
|
Apgar Scores: 1 min: |
5 min: |
|||
|
|
|
|
||||
VBAC Vacuum Forceps |
CSection ( Primary or Repeat ) |
( LTCS or Classical ) |
|||||
Maternal: |
|
|
|
Infant: |
|
|
|
||||||||
22. |
|
Have you had your postpartum check up? |
�Yes |
Date: |
24. |
Has infant |
had a newborn checkup? |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
�If No, |
when scheduled? |
|
|
|
|
|
|
If No, |
|
when scheduled? |
|||
23. |
|
Any health problems since delivery? |
�Yes |
|
�No |
|
|
If Yes, any Problems? |
|
||||||
|
If YES, please explain: |
|
|
|
25. |
|
Number of NICU Days: |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
26. |
|
Infant exposure to: (circle all that apply) |
||||
Nutrition: |
|
|
|
|
|
|
|
|
|
|
Tobacco |
Alcohol |
Drugs |
|
|
27. Maternal Dietary Assessment: For ____ Day(s) |
|
Dietary Goals: |
|
|
|
|
|
|
|||||||
|
Servs./ |
|
Suggested |
|
Client agrees to: |
|
|
|
|
||||||
Food Group |
|
Points |
|
Change |
|
|
|
|
|
|
|
|
|||
Protein |
|
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
Milk Products |
|
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
Breads/Cereals/Grains |
|
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
Vit. Crich fruit/veg |
|
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Vit. Arich fruit/veg |
|
|
+ |
|
|
|
|
REFERRALS: |
� WIC |
Date Enrolled: _________________ |
|
||||
Other fruit/veg |
|
|
+ |
|
|
|
|
� Food Stamps |
� Emergency Food |
� AFDC |
|
|
|||
Fats/Sweets |
|
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Diet adequate as assessed: |
� Yes |
� No |
Excessive: |
|
� Caffeine |
|
|
|
|
|
|
||||
28. Infant |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Method of Feeding: |
� Breast |
� Bottle |
|
|
� Breast & Bottle |
|
# Wet diapers/day? |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Type of Formula: |
|
|
With Iron? |
� Yes |
|
� No |
|
oz.. |
|
|
times/day |
||||
PsychoSocial
29. |
Do you feel comfortable in your relationship with your baby? |
� Yes |
�No |
||
|
Any special concerns? |
|
|
|
|
30. |
Are you experiencing postpartum blues? |
�Yes |
�No |
|
|
31. |
Have your household members adjusted to your baby? |
�Yes |
�No |
|
|
32. |
Has your relationship with the baby’s father changed? |
�Yes |
�No |
|
|
33.Do you have the resources to assist in maximizing the
health of you and your baby? |
|
�Yes |
�No |
|
If “No”, indicate where needs exist: �Housing |
�Financial |
�Food |
�Family � |
|
Other: |
|
|
|
|
34.Outstanding issues from Prenatal Assessment/Reassessment:
Health Education
35. If breast feeding: |
|
|
|
|
|
|
38. Do you have any questions about |
|
|
|
|
|
|
|||||||||
Do you have enough milk? |
|
|
�Yes |
�No |
|
|
|
your baby’s safety? |
|
�Yes |
�No |
|||||||||||
Do you supplement with formula? |
�Yes |
�No |
|
|
|
If “Yes”, please explain: |
|
|
|
|
|
|
||||||||||
Does your baby take the breast |
|
|
�Yes |
�No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
easily? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Are your nipples cracked and/or |
�Yes |
�No |
|
39. Are you using, or planning to use, any method of |
|||||||||||||||||
sore? |
|
|
|
|
|
|
|
|
birth |
|
|
|
|
|
|
|||||||
Do you have any questions about |
|
|
|
|
|
|
control? |
|
�Yes |
�No |
||||||||||||
|
breast feeding? |
|
|
�Yes |
�No |
|
|
|
If “Yes”, which |
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
one? |
|
|
|
|
|
|
|
||
36. Do you have any questions about |
|
|
|
|
|
|
If “No”, would you like further information? |
|
|
|
||||||||||||
mixing or feeding formula? |
|
|
�Yes |
�No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
37. Do you have any questions about your |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
baby’s health? |
|
|
�Yes |
�No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
If “Yes”, please explain: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Plan: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Client Goals, Interventions and Timeline |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Client agree to: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Referrals |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Agency: |
|
|
Date: |
|
|
|
|
Agency: |
|
|
Date: |
|
|
|
|
|||||||
Materials Given: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
�Birth Control
�___________
�Infant Feeding
�______________
�Infant Care
�___________
�Infant Safety
�___________
�
�________________________
Summary:
Date: |
|
Interviewer: |
|
Title |
|
Minutes Spent: |
Copy of Individualized Care Plan sent to Patient’s PCP on: (date) ______ by: (name and title)_______________________