|
|
|
|
|
|
|
|
|
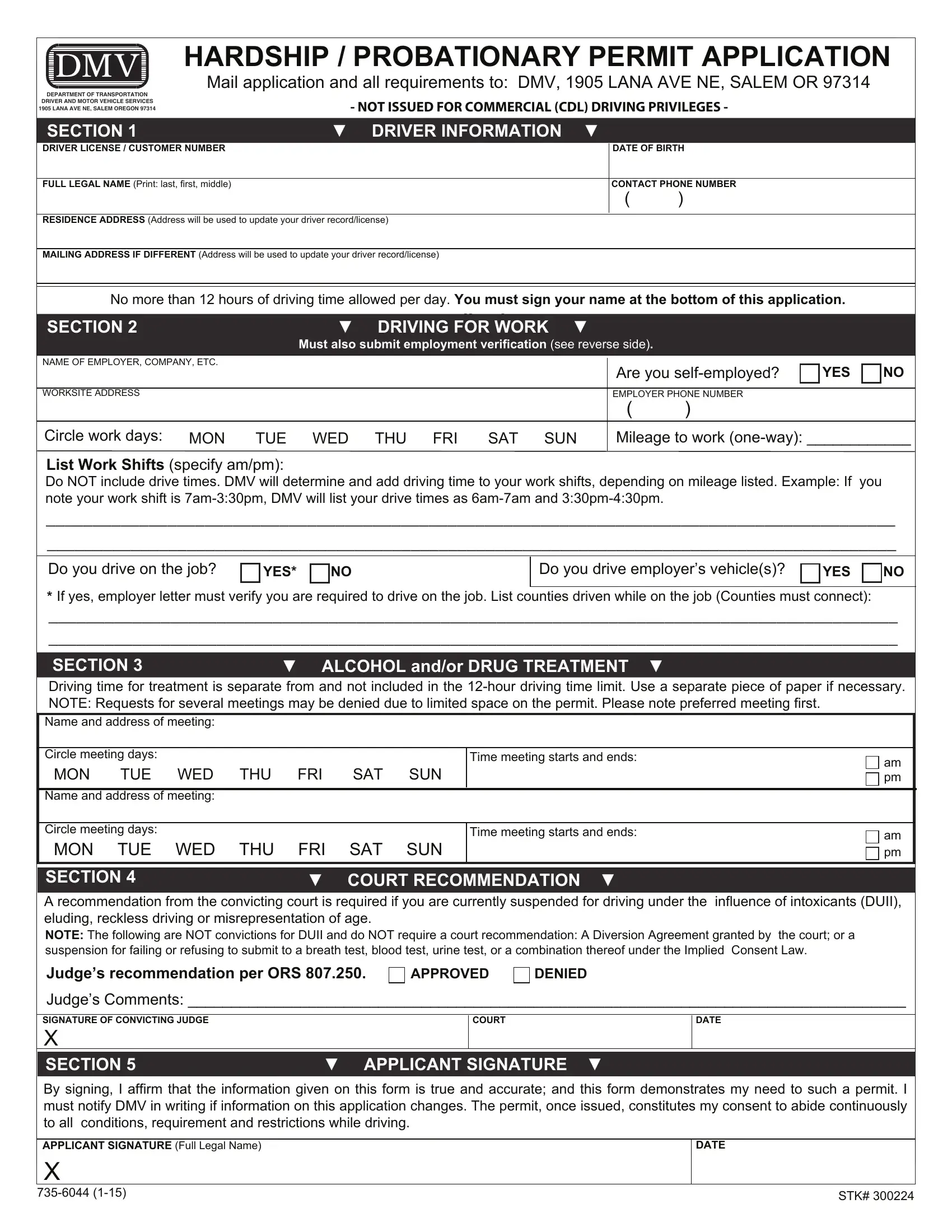
HARDSHIP / PROBATIONARY PERMIT APPLICATION |
|
|
|
|
|
|
|
|
|
|
|
|
DM V |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mail application and all requirements to: DMV, 1905 LANA AVE NE, SALEM OR 97314 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DEPARTMENT OF TRANSPORTATION |
|
DRIVER AND MOTOR VEHICLE SERVICES 1905 LANA AVE NE, SALEM OREGON 97314
- NOT ISSUED FOR COMMERCIAL (CDL) DRIVING PRIVILEGES -
SECTION 1 |
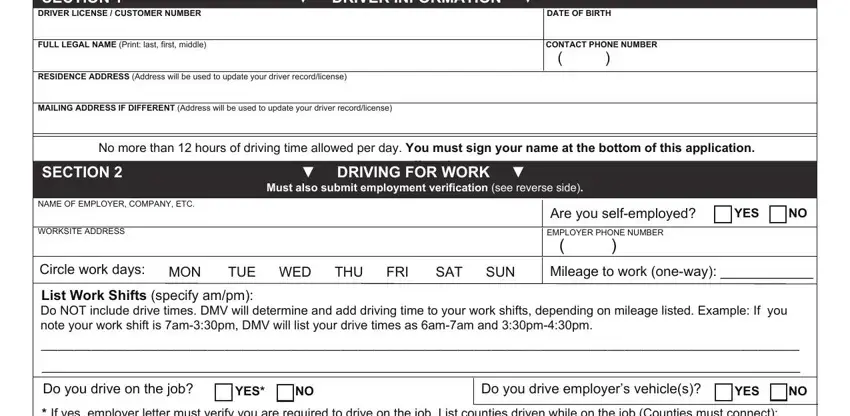
▼ DRIVER INFORMATION ▼ |
|
DRIVER LICENSE / CUSTOMER NUMBER |
|
DATE OF BIRTH |
|
|
|
FULL LEGAL NAME (Print: last, first, middle) |
|
CONTACT PHONE NUMBER |
|
|
( |
) |
|
|
|
|
RESIDENCE ADDRESS (Address will be used to update your driver record/license)
MAILING ADDRESS IF DIFFERENT (Address will be used to update your driver record/license)
No more than 12 hours of driving time allowed per day. You must sign your name at the bottom of this application.
SECTION 2 |
▼ |
application. |
▼ |
DRIVING FOR WORK |
Must also submit employment verification (see reverse side).
NAME OF EMPLOYER, COMPANY, ETC.
WORKSITE ADDRESS
Are you self-employed? |
YES |
NO |
EMPLOYER PHONE NUMBER
()
Circle work days: MON TUE WED THU FRI SAT SUN
List Work Shifts (specify am/pm):
Mileage to work (one-way): ____________
Do NOT include drive times. DMV will determine and add driving time to your work shifts, depending on mileage listed. Example: If you note your work shift is 7am-3:30pm, DMV will list your drive times as 6am-7am and 3:30pm-4:30pm.
___________________________________________________________________________________________
___________________________________________________________________________________________
Do you drive employer’s vehicle(s)?
*If yes, employer letter must verify you are required to drive on the job. List counties driven while on the job (Counties must connect):
___________________________________________________________________________________________
___________________________________________________________________________________________
SECTION 3 |
▼ ALCOHOL and/or DRUG TREATMENT ▼ |
Driving time for treatment is separate from and not included in the 12-hour driving time limit. Use a separate piece of paper if necessary. NOTE: Requests for several meetings may be denied due to limited space on the permit. Please note preferred meeting first.
Name and address of meeting:
Circle meeting days:
MON TUE WED THU FRI SAT SUN
Time meeting starts and ends: |
|
am |
|
|
|
|
|
pm |
|
|
Name and address of meeting:
Circle meeting days:
MON TUE WED THU FRI SAT SUN
Time meeting starts and ends: |
|
am |
|
|
|
|
|
pm |
|
|
SECTION 4 |
▼ COURT RECOMMENDATION ▼ |
A recommendation from the convicting court is required if you are currently suspended for driving under the influence of intoxicants (DUII), eluding, reckless driving or misrepresentation of age.
NOTE: The following are NOT convictions for DUII and do NOT require a court recommendation: A Diversion Agreement granted by the court; or a suspension for failing or refusing to submit to a breath test, blood test, urine test, or a combination thereof under the Implied Consent Law.
Judge’s recommendation per ORS 807.250.
Judge’s Comments: ___________________________________________________________________________________
SIGNATURE OF CONVICTING JUDGE
X
SECTION 5 |
▼ APPLICANT SIGNATURE ▼ |
By signing, I affirm that the information given on this form is true and accurate; and this form demonstrates my need to such a permit. I must notify DMV in writing if information on this application changes. The permit, once issued, constitutes my consent to abide continuously to all conditions, requirement and restrictions while driving.
APPLICANT SIGNATURE (Full Legal Name)
X
735-6044 (1-15) |
STK# 300224 |
|
DMV field offices cannot process the application. Hardship/probationary permits are subject to the fees, provisions, conditions, prohibitions and penalties applicable to a license, including Oregon residency and no suspensions in any other state.
REQUIRMENTS FOR ALL HARDSHIP/PROBATIONARY PERMITS
Application (completed and signed)
Fees
Application Fee…………..…… $ 50 (Non-refundable ORS 807.240(6))
Reinstatement Fee………..….. $ 75
TOTAL $125 (Check or money order)
SR22 Insurance Certificate
Have an automobile insurance company file an Oregon SR-22 certificate with DMV. Must be the original SR22 (no copies or faxes). DMV will not issue the permit until the SR22 becomes effective.
Employment Verification
If employed, submit a letter from your employer verifying employment: on company letterhead; signed and dated; listing days and hours of employment; and stating need to drive on the job, if required.
If self-employed, submit a copy of your current business license (must show your name and business name); a copy of your signed tax statement for the preceding year; or two other documents such as a current customer signed business receipt, advertisements, signed contracts, signed and dated letters from customers, etc.
If unemployed, submit the days, hours and counties you drive to seek employment.
ADDITIONAL REQUIREMENTS
You may have additional requirements if you have been convicted of Driving Under the Influence of Intoxicants, revoked as a Habitual Offender, etc. Call DMV at (503) 945-5000 to determine if any additional requirements are needed.
Are you revoked for Habitual Offender?
If yes, you must complete a Medical (Diagnostic) Exam. To meet the eligibility requirements for a Medical (Diagnostic) Exam, your physician must complete and sign this medical statement. (Do not send DMV a copy of the actual Medical Exam.) If you are not able to obtain a doctor’s signature on this medical statement, call the Driver Safety Unit at (503) 945-5083 to obtain a Driver Medical Report form for your doctor to complete.
PATIENT’S LAST NAME (Please Print) |
FIRST NAME |
MIDDLE NAME |
DATE OF BIRTH |
|
|
|
|
I have taken a medical history and completed a physical exam on the above named patient. In my opinion, the patient does not |
DATE OF EXAM (Month, Day, Year) |
have a physical or mental condition or impairment that affects the patient’s ability to safely operate a motor vehicle. |
|
|
|
|
|
MEDICAL PROVIDER NAME (Please Print) |
SPECIALTY |
LICENSE OR CERTIFICATE # |
|
|
|
MAILING ADDRESS (City, State, ZIP Code) |
TELEPHONE NUMBER |
FAX NUMBER |
|
( |
) |
( |
) |
SIGNATURE OF MEDICAL PROVIDER |
|
|
DATE SIGNED |
X |
|
|
|
|
Are you suspended ONLY for an uninsured accident or misrepresentation of age?
If yes, you may be eligible for the following driving privileges: medical appointments, grocery shopping, child care, school and to care for elderly family members. Call DMV at (503) 945-5000 to determine if you are eligible for additional driving privileges and to obtain a list of required information to submit with your request.
WHAT’S NEXT?
The Driver Suspension Unit will review your application and notify you of any additional requirements you must complete before a permit can be issued. If you have additional requirements and you do not comply with all requirements within 60 days, your application will be denied and you will need to re-apply for the permit, which includes submitting all new documents and $50 application fee.
Once your application is approved and all requirements are met, DMV will mail you a restriction letter. Take the restriction letter to a DMV field office to obtain a restricted driver license. Your driving privileges are not valid until you have obtained both the restriction letter mailed from Headquarters and a driver license with a “J” restriction code issued at a field office.