
Writing the center of hope wichita ks document is not difficult using our PDF editor. Keep up with these particular actions to get the document ready without delay.
Step 1: Choose the orange "Get Form Now" button on the following website page.
Step 2: Now you are ready to edit center of hope wichita ks. You possess a wide range of options with our multifunctional toolbar - it's possible to add, delete, or change the information, highlight the specified elements, and perform similar commands.
Enter the data demanded by the platform to create the form.
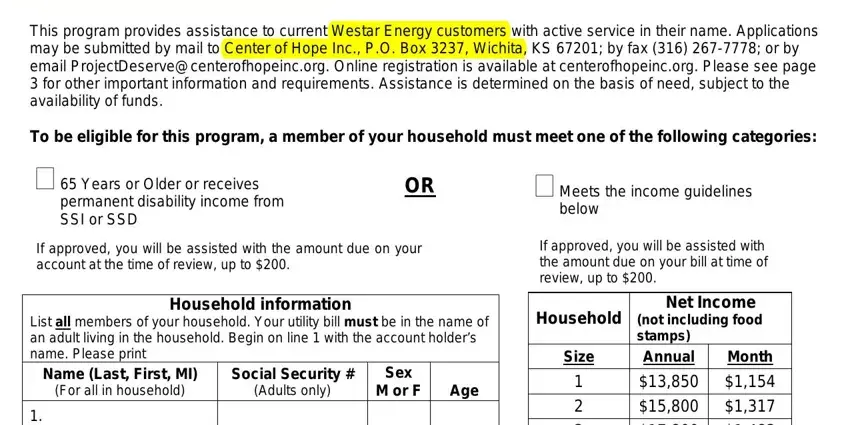
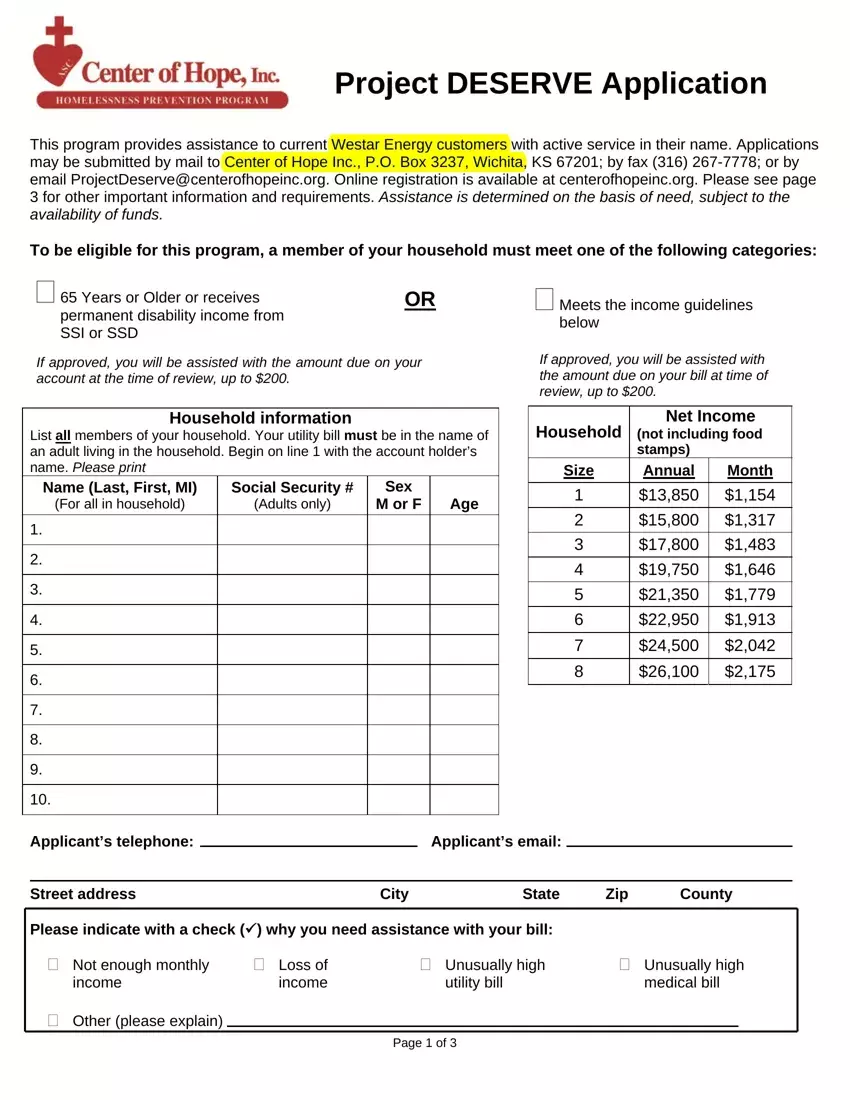
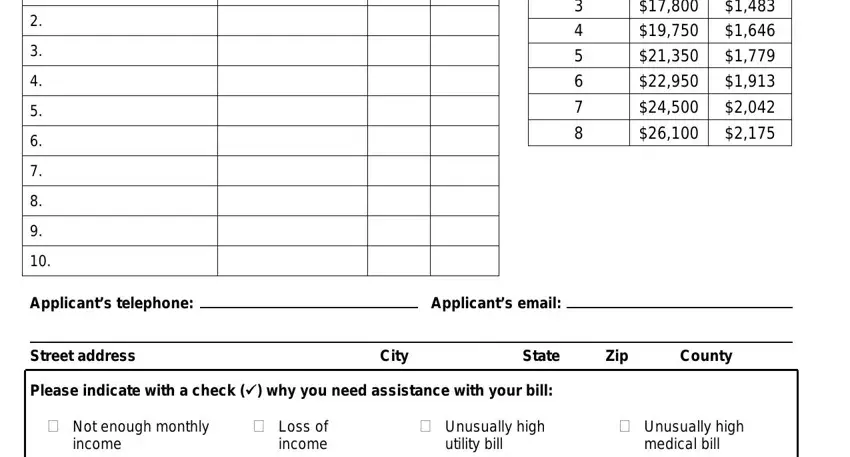
Type in the necessary particulars in the segment Applicants telephone, Applicants email, Street address, City, State, Zip, County, Please indicate with a check why, cid Not enough monthly, income, cid Loss of income, cid Unusually high utility bill, and cid Unusually high medical bill.
In the section discussing cid Other please explain, and Page of, it's essential to write down some essential particulars.

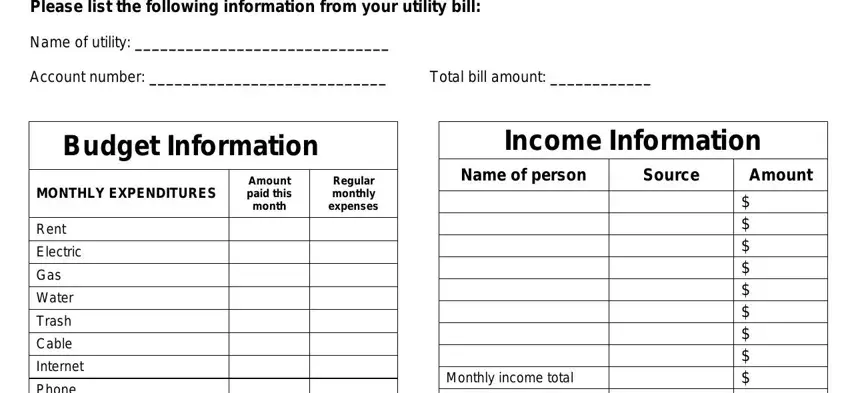
The Please list the following, Name of utility, Account number, Total bill amount, Budget Information, MONTHLY EXPENDITURES, Amount paid this month, Regular monthly expenses, Rent, Electric, Gas, Water, Trash, Cable, and Internet section allows you to specify the rights and responsibilities of each party.
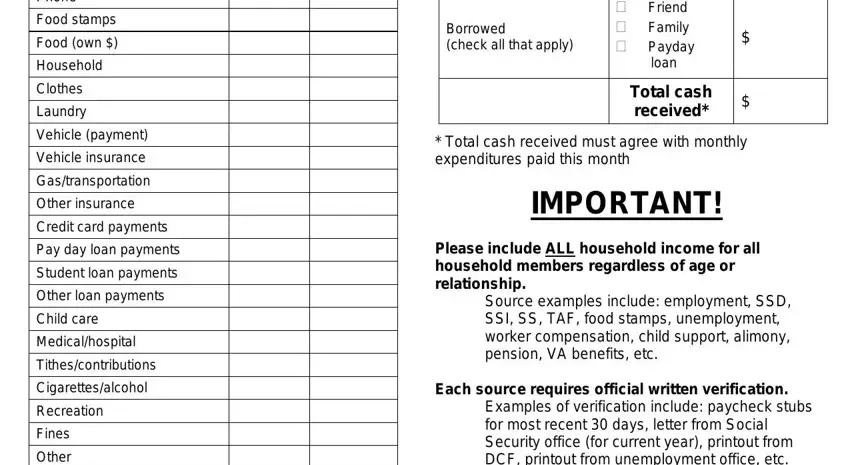
Check the sections Phone, Food stamps, Food own, Household, Clothes, Laundry, Vehicle payment, Vehicle insurance, Gastransportation, Other insurance, Credit card payments, Pay day loan payments, Student loan payments, Other loan payments, and Child care and thereafter fill them out.
Step 3: Hit the button "Done". Your PDF form can be transferred. It is possible to obtain it to your device or send it by email.
Step 4: To stay away from potential future concerns, make sure you possess up to two or more duplicates of each document.
