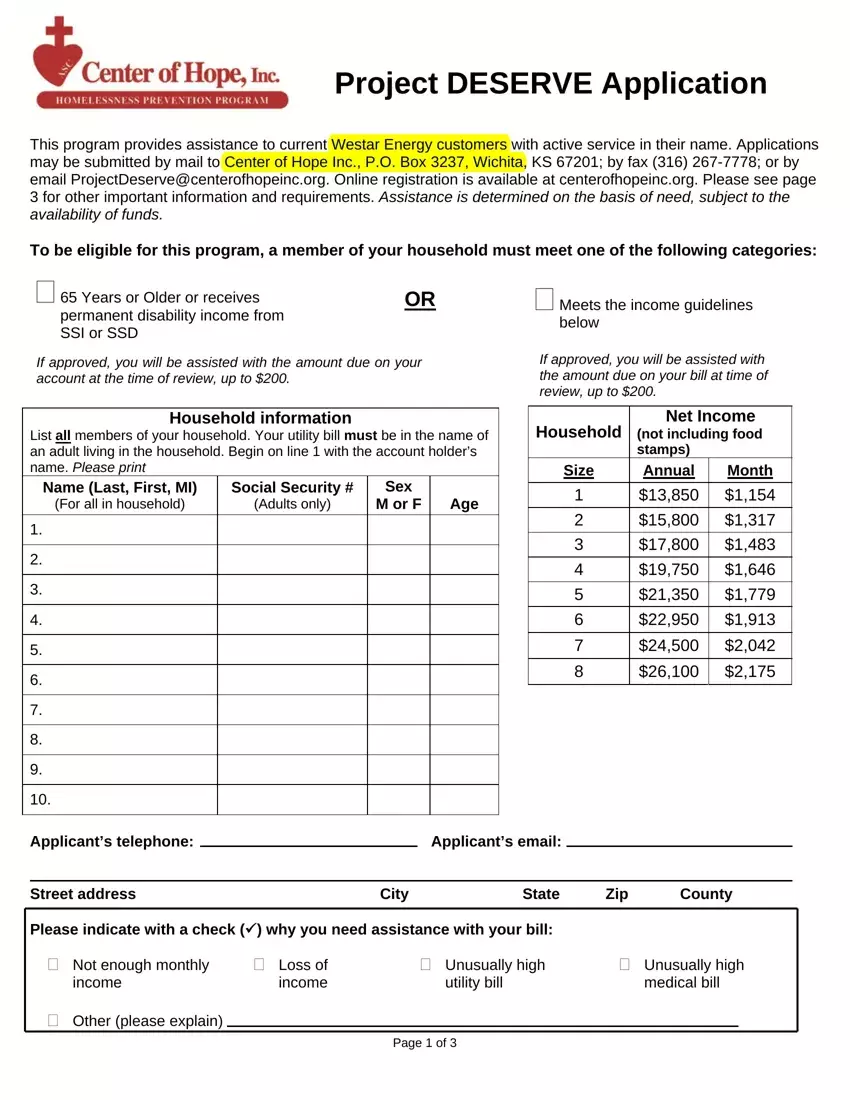
The Project DESERVE Application form is an essential tool for Westar Energy customers in need of financial assistance with their utility bills. Designed to support individuals based on their financial necessity, the program accepts applications through various channels including mail, fax, and email, as well as offers online registration options. Eligibility hinges on certain criteria, such as age, disability, or meeting specific income guidelines, ensuring assistance reaches those who need it most, with benefits up to $200 towards the account balance at the time of review. Applicants are required to provide comprehensive household information, including details of all income sources and monthly expenditures, alongside the necessary verification documents to substantiate their application. The form meticulously outlines what constitutes as valid income verification and emphasizes the importance of submitting copies rather than original documents, all of which will be securely destroyed post-review. Furthermore, it sets clear expectations regarding the submission process, required documentation, and the timeframe within which applicants can expect to receive a decision, underlying the program's commitment to transparency and assistance for individuals facing financial challenges.
| Question | Answer |
|---|---|
| Form Name | Project Deserve Application |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | project deserve application, project deserve topeka, center of hope, project deserve application wichita ks |
