This PDF editor enables you to fill in forms. You should not undertake much to update florida bluecross provider form documents. Merely adhere to these actions.
Step 1: Choose the "Get Form Here" button.
Step 2: After you have entered the florida blue provider enrollment application edit page, you'll discover all functions you may undertake regarding your document within the upper menu.
Get the florida blue provider enrollment application PDF and type in the content for every single segment:
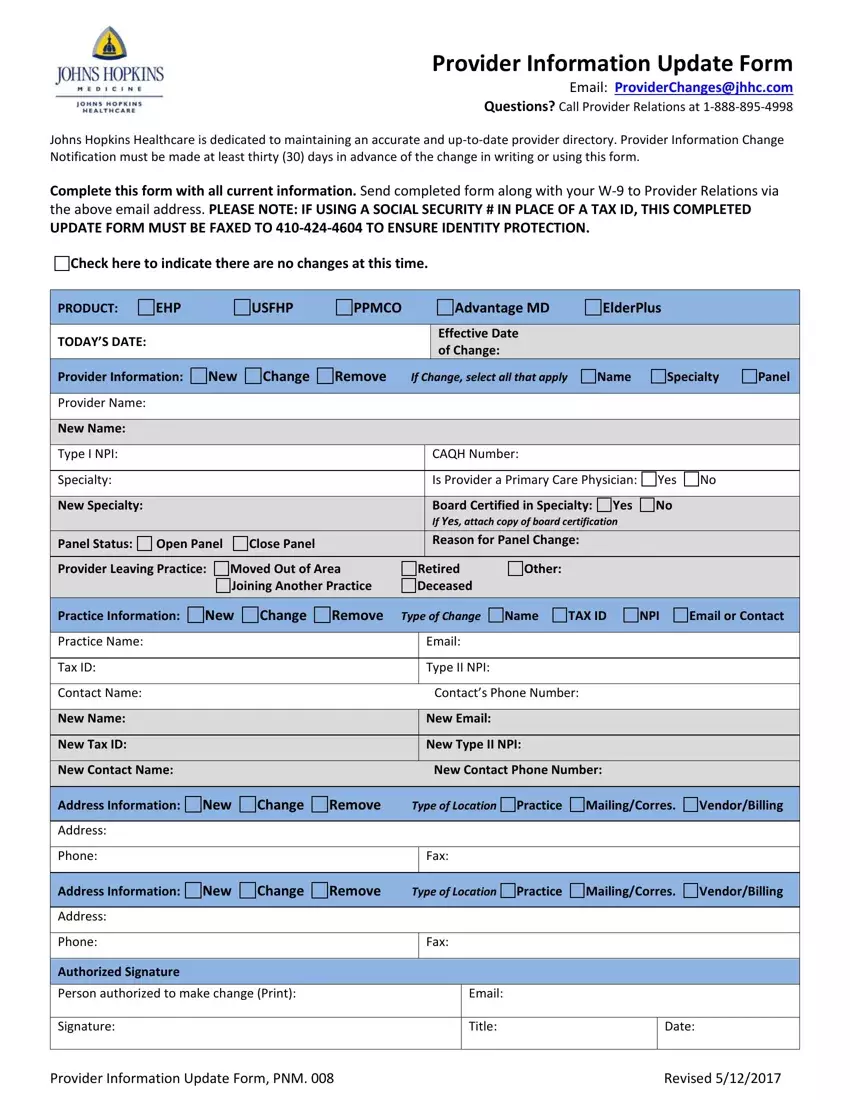
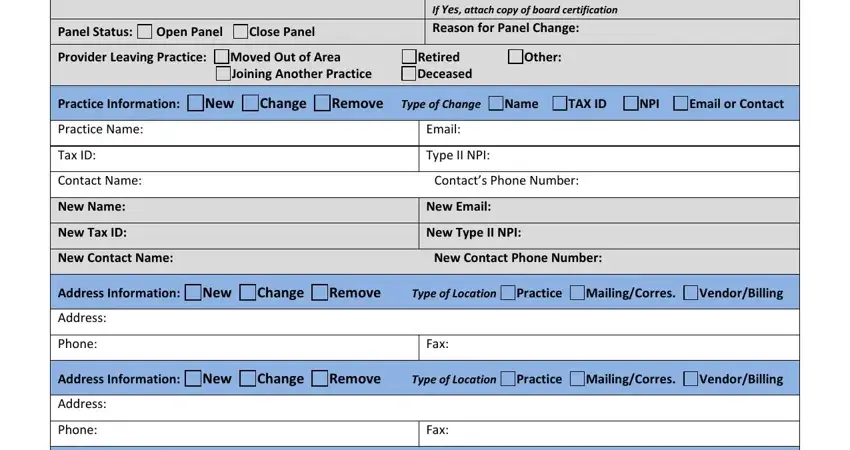
Fill out the New Specialty, Panel Status, Open Panel, Close Panel, Board Certified in Specialty If, Yes No, Provider Leaving Practice Moved, Retired Other, Joining Another Practice Deceased, Practice Information New, Change, Remove Type of Change Name, TAX ID NPI, Email or Contact, and Practice Name section with all the details asked by the platform.
In the Authorized Signature, Person authorized to make change, Signature, Email, Title, Date, Provider Information Update Form, and Revised area, identify the key details.

Step 3: Hit the button "Done". Your PDF form can be transferred. You can upload it to your device or email it.
Step 4: To protect yourself from different problems in the foreseeable future, try to get a minimum of a couple of copies of your form.
