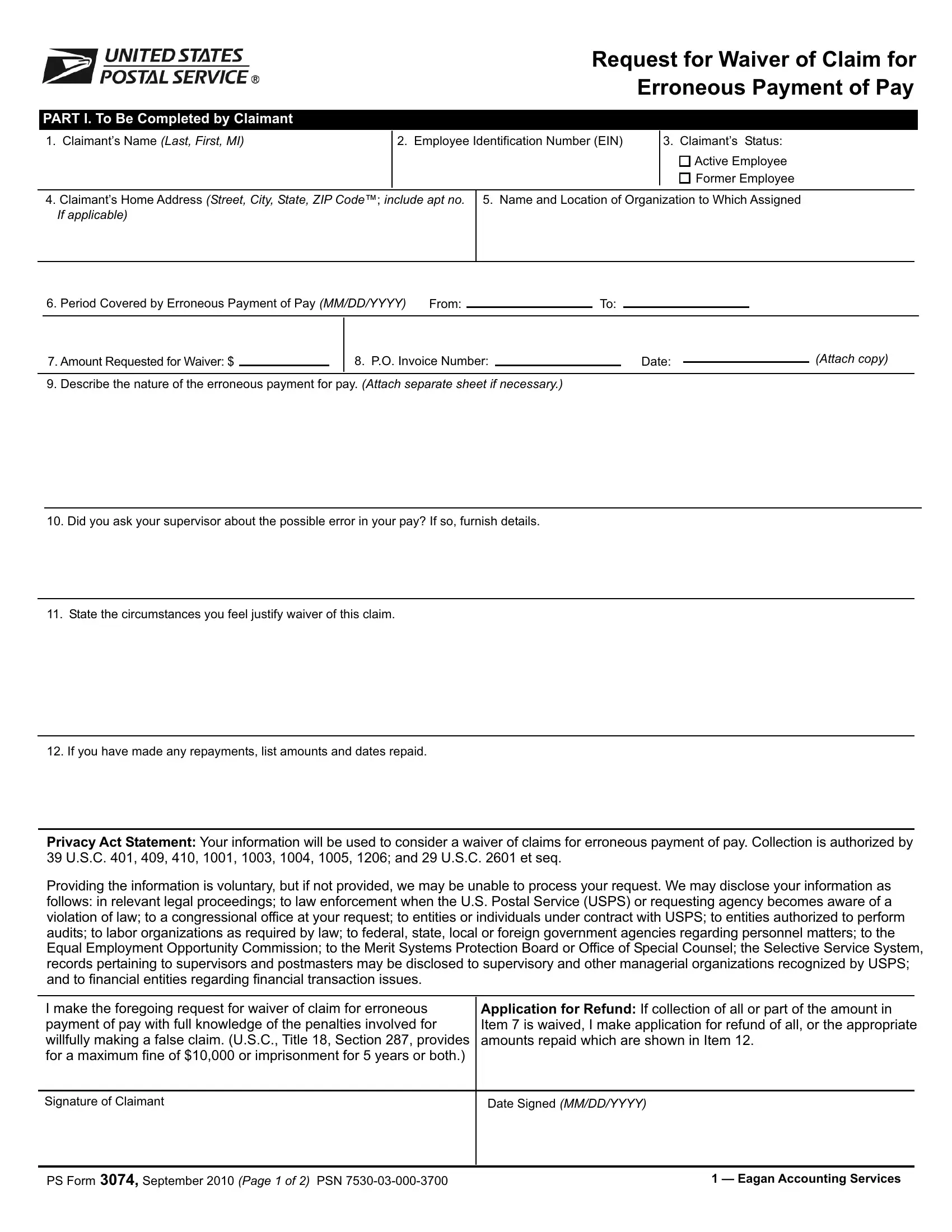
The PS 3074 form serves a critical role within the procedures of managing employment-related financial discrepancies, specifically focusing on the waiver of claims for erroneous payment of pay. It is a comprehensive document meticulously designed to not only identify the claimant by requiring detailed personal and employment information but also to pinpoint the nature and period of the erroneous payment. Claimants are walked through a systematic process that begins with their personal identification, attaching to their employment status and further extending into the specifics of the erroneous payment including the amount and the circumstances that led to its occurrence. The form also acts as a platform for claimants to justify the request for a waiver, requiring them to articulate their reasons, query their supervisors, and note any repayments made. Critical to the form’s integrity is the Privacy Act Statement, highlighting its adherence to legal stipulations governing the collection, use, and disclosure of personal information. Furthermore, the multi-part structure of the form extends beyond the claimant’s declaration, incorporating assessments and certifications from responsible postal or employment authorities, ensuring a thorough evaluation process. Such detailed procedural steps underscore not only the importance of accuracy and completeness in addressing financial rectifications but also the legal and ethical considerations at play in managing employment compensation issues. Overall, the PS 3074 form embodies the intersection of organizational accountability, employee rights, and the regulatory framework that governs employment practices.
| Question | Answer |
|---|---|
| Form Name | Ps Form 3074 |
| Form Length | 6 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 30 sec |
| Other names | 3074 pdf form, usps form ps 3074, ps 3074 form, mm erroneous dd |
Request for Waiver of Claim for
Erroneous Payment of Pay
PART I. To Be Completed by Claimant
1. Claimant’s Name (Last, First, MI) |
2. Employee Identification Number (EIN) |
3. Claimant’s Status: |
|
|
|
|
Active Employee |
|
|
|
Former Employee |
|
|
|
|
4. Claimant’s HomeAddress (Street, City, State, ZIPCode™; include apt no. |
5. Name and Location of Organization to WhichAssigned |
||
If applicable) |
|
|
|
|
|
|
|
|
6. Period Covered by Erroneous Payment of Pay (MM/DD/YYYY) |
From: |
|
To: |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7.Amount Requested for Waiver: $ |
|
|
8. P.O. Invoice Number: |
|
|
|
Date: |
|
|
(Attach copy) |
|
||
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9. Describe the nature of the erroneous payment for pay. (Attach separate sheet if necessary.) |
|
|
|
|
|
|
|
||||||
10.Did you ask your supervisor about the possible error in your pay? If so, furnish details.
11.State the circumstances you feel justify waiver of this claim.
12. If you have made any repayments, list amounts and dates repaid.
PrivacyAct Statement:Your information will be used to consider a waiver of claims for erroneous payment of pay. Collection is authorized by 39 U.S.C. 401, 409, 410, 1001, 1003, 1004, 1005, 1206; and 29 U.S.C. 2601 et seq.
Providing the information is voluntary, but if not provided, we may be unable to process your request. We may disclose your information as follows: in relevant legal proceedings; to law enforcement when the U.S. Postal Service (USPS) or requesting agency becomes aware of a violation of law; to a congressional office at your request; to entities or individuals under contract with USPS; to entities authorized to perform audits; to labor organizations as required by law; to federal, state, local or foreign government agencies regarding personnel matters; to the Equal Employment Opportunity Commission; to the Merit Systems Protection Board or Office of Special Counsel; the Selective Service System, records pertaining to supervisors and postmasters may be disclosed to supervisory and other managerial organizations recognized by USPS; and to financial entities regarding financial transaction issues.
I make the foregoing request for waiver of claim for erroneous payment of pay with full knowledge of the penalties involved for willfully making a false claim. (U.S.C., Title 18, Section 287, provides for a maximum fine of $10,000 or imprisonment for 5 years or both.)
Application for Refund: If collection of all or part of the amount in Item 7 is waived, I make application for refund of all, or the appropriate amounts repaid which are shown in Item 12.
Signature of Claimant
Date Signed (MM/DD/YYYY)
PS Form 3074,September 2010 (Page 1 of 2) PSN |
1 — EaganAccounting Services |
PART II. To Be Completed by Current Postmaster or Installation Head of theActive or Former Employee
(Retain one copy. Forward original and one copy to Manager, Human Resources (District).
Provide all additional facts or circumstances that will clairfy and amplify the statement of facts made by the claimant on the claim form, including a descritpion of how the overpayment occurred. (Continue on separate sheet, if necessary)
GrossAmount of Claim Listed by Pay Periods
Pay |
|
Amount |
Pay |
|
Amount |
Pay |
|
Amount |
Period |
Amount Paid |
Should Be |
Period |
Amount Paid |
Should Be |
Period |
Amount Paid |
Should Be |
|
|
|
|
|
|
|
|
|
$ |
$ |
|
$ |
$ |
|
|
$ |
$ |
$ |
$ |
|
$ |
$ |
|
|
$ |
$ |
$ |
$ |
|
$ |
$ |
|
|
$ |
$ |
To the best of my knowledge and belief there is no indication of fraud, misrepresentation fault, or lack of good faith on the part of the claimant or any other person having an interest in this request for waiver of claim.
Signature |
Title |
Date (MM/DD/YYYY) |
|
|
|
Printed Name |
Phone Number |
|
PART III. To Be Completed by Manager, Human Resources (District).
(Retain one copy. Forward original to EaganAccounting Services.)
Review form for accuracy and completeness.Add any additional pertinent facts. (Continue on separate sheet, if necessary.)
Signature |
Title |
Date (MM/DD/YYYY) |
|
|
|
Printed Name |
Phone Number |
|
PART IV. To Be Completed by Manager, EaganAccounting Services.
GrossAmount Claimed |
$ |
ClaimAllowed |
|
|
|
|
|
GrossAmount Waived |
$ |
ClaimDenied |
|
|
|
||
|
|
|
|
Signature |
Title |
|
Date (MM/DD/YYYY) |
Printed Name
Phone Number
MAIL TO:ACCOUNTING SERVICES, 2825 LONE OAK PKWY, EAGAN MN
PS Form 3074,September 2010 (Page 2 of 2) PSN
Request for Waiver of Claim for
Erroneous Payment of Pay
PART I. To Be Completed by Claimant
1. Claimant’s Name (Last, First, MI) |
2. Employee Identification Number (EIN) |
3. Claimant’s Status: |
|
|
|
|
Active Employee |
|
|
|
Former Employee |
|
|
|
|
4. Claimant’s HomeAddress (Street, City, State, ZIPCode™; include apt no. |
5. Name and Location of Organization to WhichAssigned |
||
If applicable) |
|
|
|
|
|
|
|
|
6. Period Covered by Erroneous Payment of Pay (MM/DD/YYYY) |
From: |
|
To: |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7.Amount Requested for Waiver: $ |
|
|
8. P.O. Invoice Number: |
|
|
|
Date: |
|
|
(Attach copy) |
|
||
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9. Describe the nature of the erroneous payment for pay. (Attach separate sheet if necessary.) |
|
|
|
|
|
|
|
||||||
10.Did you ask your supervisor about the possible error in your pay? If so, furnish details.
11.State the circumstances you feel justify waiver of this claim.
12. If you have made any repayments, list amounts and dates repaid.
PrivacyAct Statement:Your information will be used to consider a waiver of claims for erroneous payment of pay. Collection is authorized by 39 U.S.C. 401, 409, 410, 1001, 1003, 1004, 1005, 1206; and 29 U.S.C. 2601 et seq.
Providing the information is voluntary, but if not provided, we may be unable to process your request. We may disclose your information as follows: in relevant legal proceedings; to law enforcement when the U.S. Postal Service (USPS) or requesting agency becomes aware of a violation of law; to a congressional office at your request; to entities or individuals under contract with USPS; to entities authorized to perform audits; to labor organizations as required by law; to federal, state, local or foreign government agencies regarding personnel matters; to the Equal Employment Opportunity Commission; to the Merit Systems Protection Board or Office of Special Counsel; the Selective Service System, records pertaining to supervisors and postmasters may be disclosed to supervisory and other managerial organizations recognized by USPS; and to financial entities regarding financial transaction issues.
I make the foregoing request for waiver of claim for erroneous payment of pay with full knowledge of the penalties involved for willfully making a false claim. (U.S.C., Title 18, Section 287, provides for a maximum fine of $10,000 or imprisonment for 5 years or both.)
Application for Refund: If collection of all or part of the amount in Item 7 is waived, I make application for refund of all, or the appropriate amounts repaid which are shown in Item 12.
Signature of Claimant
Date Signed (MM/DD/YYYY)
PS Form 3074,September 2010 (Page 1 of 2) PSN |
2 — Manager, Human Resources |
PART II. To Be Completed by Current Postmaster or Installation Head of theActive or Former Employee
(Retain one copy. Forward original and one copy to Manager, Human Resources (District).
Provide all additional facts or circumstances that will clairfy and amplify the statement of facts made by the claimant on the claim form, including a descritpion of how the overpayment occurred. (Continue on separate sheet, if necessary)
GrossAmount of Claim Listed by Pay Periods
Pay |
|
Amount |
Pay |
|
Amount |
Pay |
|
Amount |
Period |
Amount Paid |
Should Be |
Period |
Amount Paid |
Should Be |
Period |
Amount Paid |
Should Be |
$ |
$ |
|
$ |
$ |
|
|
$ |
$ |
$ |
$ |
|
$ |
$ |
|
|
$ |
$ |
$ |
$ |
|
$ |
$ |
|
|
$ |
$ |
To the best of my knowledge and belief there is no indication of fraud, misrepresentation fault, or lack of good faith on the part of the claimant or any other person having an interest in this request for waiver of claim.
Signature |
Title |
Date (MM/DD/YYYY) |
|
|
|
Printed Name |
Phone Number |
|
PART III. To Be Completed by Manager, Human Resources (District).
(Retain one copy. Forward original to EaganAccounting Services.)
Review form for accuracy and completeness.Add any additional pertinent facts. (Continue on separate sheet, if necessary.)
Signature |
Title |
Date (MM/DD/YYYY) |
|
|
|
Printed Name |
Phone Number |
|
PART IV. To Be Completed by Manager, EaganAccounting Services.
GrossAmount Claimed |
$ |
ClaimAllowed |
|
|
|
|
|
GrossAmount Waived |
$ |
ClaimDenied |
|
|
|
||
|
|
|
|
Signature |
Title |
|
Date (MM/DD/YYYY) |
Printed Name
Phone Number
MAIL TO:ACCOUNTING SERVICES, 2825 LONE OAK PKWY, EAGAN MN
PS Form 3074,September 2010 (Page 2 of 2) PSN
Request for Waiver of Claim for
Erroneous Payment of Pay
PART I. To Be Completed by Claimant
1. Claimant’s Name (Last, First, MI) |
2. Employee Identification Number (EIN) |
3. Claimant’s Status: |
|
|
|
|
Active Employee |
|
|
|
Former Employee |
|
|
|
|
4. Claimant’s HomeAddress (Street, City, State, ZIPCode™; include apt no. |
5. Name and Location of Organization to WhichAssigned |
||
If applicable) |
|
|
|
|
|
|
|
|
6. Period Covered by Erroneous Payment of Pay (MM/DD/YYYY) |
From: |
|
To: |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7.Amount Requested for Waiver: $ |
|
|
8. P.O. Invoice Number: |
|
|
|
Date: |
|
|
(Attach copy) |
|
||
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9. Describe the nature of the erroneous payment for pay. (Attach separate sheet if necessary.) |
|
|
|
|
|
|
|
||||||
10.Did you ask your supervisor about the possible error in your pay? If so, furnish details.
11.State the circumstances you feel justify waiver of this claim.
12. If you have made any repayments, list amounts and dates repaid.
PrivacyAct Statement:Your information will be used to consider a waiver of claims for erroneous payment of pay. Collection is authorized by 39 U.S.C. 401, 409, 410, 1001, 1003, 1004, 1005, 1206; and 29 U.S.C. 2601 et seq.
Providing the information is voluntary, but if not provided, we may be unable to process your request. We may disclose your information as follows: in relevant legal proceedings; to law enforcement when the U.S. Postal Service (USPS) or requesting agency becomes aware of a vio- lation of law; to a congressional office at your request; to entities or individuals under contract with USPS; to entities authorized to perform au- dits; to labor organizations as required by law; to federal, state, local or foreign government agencies regarding personnel matters; to the Equal Employment Opportunity Commission; to the Merit Systems Protection Board or Office of Special Counsel; the Selective Service System, records pertaining to supervisors and postmasters may be disclosed to supervisory and other managerial organizations recognized by USPS; and to financial entities regarding financial transaction issues.
I make the foregoing request for waiver of claim for erroneous payment of pay with full knowledge of the penalties involved for willfully making a false claim. (U.S.C., Title 18, Section 287, provides for a maximum fine of $10,000 or imprisonment for 5 years or both.)
Application for Refund: If collection of all or part of the amount in Item 7 is waived, I make application for refund of all, or the appropriate amounts repaid which are shown in Item 12.
Signature of Claimant
Date Signed (MM/DD/YYYY)
PS Form 3074,September 2010 (Page 1 of 2) PSN |
3 — Installation Head |
PART II. To Be Completed by Current Postmaster or Installation Head of theActive or Former Employee
(Retain one copy. Forward original and one copy to Manager, Human Resources (District).
Provide all additional facts or circumstances that will clairfy and amplify the statement of facts made by the claimant on the claim form, including a descritpion of how the overpayment occurred. (Continue on separate sheet, if necessary)
GrossAmount of Claim Listed by Pay Periods
Pay |
|
Amount |
Pay |
|
Amount |
Pay |
|
Amount |
Period |
Amount Paid |
Should Be |
Period |
Amount Paid |
Should Be |
Period |
Amount Paid |
Should Be |
$ |
$ |
|
$ |
$ |
|
|
$ |
$ |
$ |
$ |
|
$ |
$ |
|
|
$ |
$ |
$ |
$ |
|
$ |
$ |
|
|
$ |
$ |
To the best of my knowledge and belief there is no indication of fraud, misrepresentation fault, or lack of good faith on the part of the claimant or any other person having an interest in this request for waiver of claim.
Signature |
Title |
Date (MM/DD/YYYY) |
|
|
|
Printed Name |
Phone Number |
|
PART III. To Be Completed by Manager, Human Resources (District).
(Retain one copy. Forward original to EaganAccounting Services.)
Review form for accuracy and completeness.Add any additional pertinent facts. (Continue on separate sheet, if necessary.)
Signature |
Title |
Date (MM/DD/YYYY) |
|
|
|
Printed Name |
Phone Number |
|
PART IV. To Be Completed by Manager, EaganAccounting Services.
GrossAmount Claimed |
$ |
ClaimAllowed |
|
|
|
|
|
GrossAmount Waived |
$ |
ClaimDenied |
|
|
|
||
|
|
|
|
Signature |
Title |
|
Date (MM/DD/YYYY) |
Printed Name
Phone Number
MAIL TO:ACCOUNTING SERVICES, 2825 LONE OAK PKWY, EAGAN MN
PS Form 3074,September 2010 (Page 2 of 2) PSN