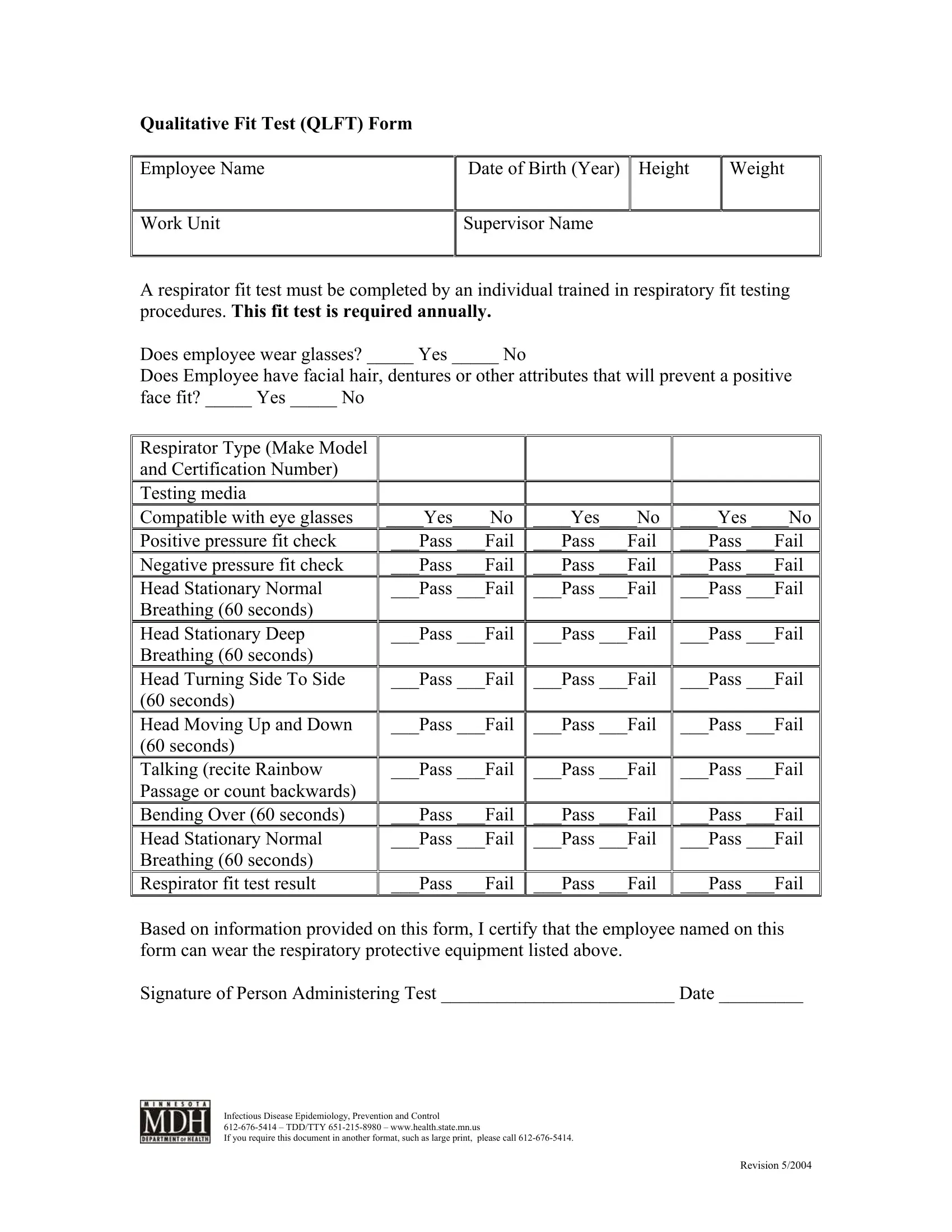
In the realm of occupational health and safety, ensuring that employees are provided with the right protective equipment that fits correctly is not just a matter of compliance, but a fundamental aspect of safeguarding their wellbeing. Among the variety of tests and procedures in place to fulfill this objective, the Qualitative Fit Test (QLFT) stands out as a pivotal measure. The QLFT Form is a meticulously organized document that serves as a record for the fit testing of respiratory protective equipment. Required annually, this form captures essential information starting from the employee's name, date of birth, height, and weight, to more specific details concerning the make, model, and certification number of the respirator being tested. It accounts for individual factors that may affect the fit, such as the presence of glasses, facial hair, or dentures. The form delineates a series of conditions under which the respirator's fit is tested, including different head movements and breathing patterns, to ensure the equipment's effectiveness across a wide range of scenarios. Accordingly, the fit test is marked with a pass or fail for each condition, culminating in a certification that endorses the employee's ability to wear the prescribed protective gear. Moreover, the form is not just a record; it is a testament to the commitment of employers to the health and safety of their employees, underscored by the signature of the person administering the test and supported by contact information for infectious disease epidemiology, prevention, and control. The QLFT Form, thus, embodies a crucial intersection of regulatory compliance, safety standards, and employee health protection.
| Question | Answer |
|---|---|
| Form Name | Qlft Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Administering, 2004, qlft, TTY |
