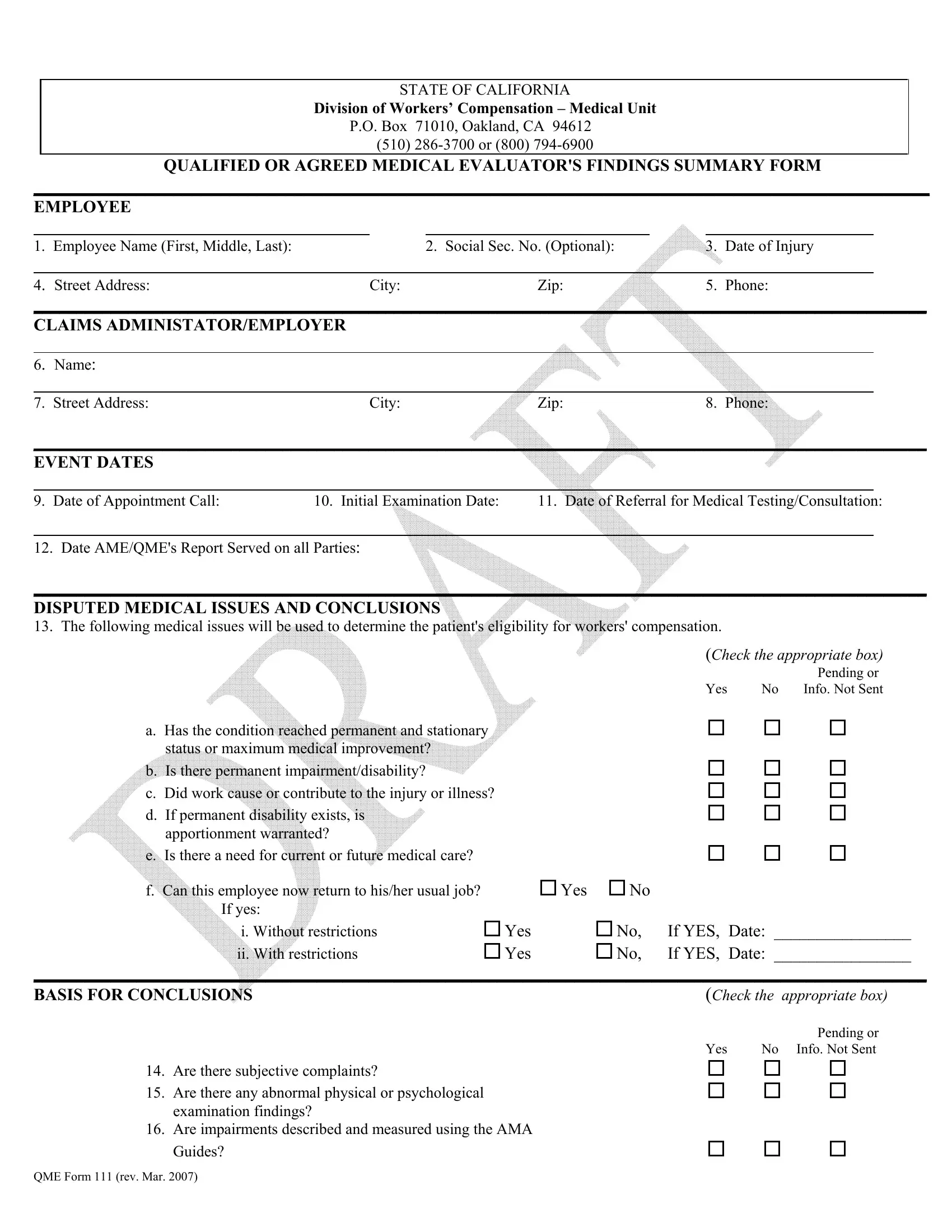
The QME 111 form, an essential document within the California workers' compensation system, outlines the findings of a Qualified or Agreed Medical Evaluator regarding an employee's work-related injury or illness. This comprehensive form, curated by the State of California Division of Workers’ Compensation – Medical Unit, serves as a critical communication tool between medical evaluators, employees, and claims administrators or employers. It meticulously captures a range of details including personal information about the employee, specifics about the claims administrator or employer, crucial event dates like the appointment call and initial examination, along with disputed medical issues and the evaluator’s conclusions. Additionally, it is instrumental in documenting the process of medical evaluation through listings of subjective complaints, abnormal findings, diagnostic test results, and the crucial utilization of the AMA Guides for determining impairment. The form also details the review of medical records and consultations with other physicians, culminating in the QME or AME's signed declaration. Satisfying legal requirements, this form is designed to ensure clear, concise, and transparent communication of an employee's medical evaluation findings, facilitating the determination of eligibility for workers' compensation benefits. By providing a structured summary of the evaluator's findings, it supports the fair and efficient resolution of workers' compensation claims, making it a pivotal document for all parties involved in the adjudication process.
| Question | Answer |
|---|---|
| Form Name | Qme Form 111 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | thereon, DEU, ADMINISTATOR, qualified or agreed medical evaluator's findings summary form fill in |
STATE OF CALIFORNIA
Division of Workers’ Compensation – Medical Unit
P.O. Box 71010, Oakland, CA 94612
(510)
QUALIFIED OR AGREED MEDICAL EVALUATOR'S FINDINGS SUMMARY FORM
________________________________________________________________________________________________
EMPLOYEE
1. |
Employee Name (First, Middle, Last): |
2. |
Social Sec. No. (Optional): |
3. |
Date of Injury |
|
|
|
|
|
|
4. |
Street Address: |
City: |
Zip: |
5. |
Phone: |
________________________________________________________________________________________________________
CLAIMS ADMINISTATOR/EMPLOYER
6. |
Name: |
|
|
|
|
|
|
|
|
7. |
Street Address: |
City: |
Zip: |
8. Phone: |
________________________________________________________________________________________________________
EVENT DATES
9. Date of Appointment Call: |
10. Initial Examination Date: |
11. Date of Referral for Medical Testing/Consultation: |
12. Date AME/QME's Report Served on all Parties:
________________________________________________________________________________________________________
DISPUTED MEDICAL ISSUES AND CONCLUSIONS
13. The following medical issues will be used to determine the patient's eligibility for workers' compensation.
(Check the appropriate box)
|
|
Pending or |
Yes |
No |
Info. Not Sent |
a. Has the condition reached permanent and stationary status or maximum medical improvement?
b. Is there permanent impairment/disability?
c. Did work cause or contribute to the injury or illness?
d. If permanent disability exists, is apportionment warranted?
e. Is there a need for current or future medical care?
f. Can this employee now return to his/her usual job? |
Yes |
No |
|
|
If yes: |
|
|
|
|
i. Without restrictions |
Yes |
No, |
If YES, |
Date: ________________ |
ii. With restrictions |
Yes |
No, |
If YES, |
Date: ________________ |
________________________________________________________________________________________________________
BASIS FOR CONCLUSIONS |
(Check the |
appropriate box) |
|
|
|
|
Pending or |
|
Yes |
No |
Info. Not Sent |
14. Are there subjective complaints?
15. Are there any abnormal physical or psychological examination findings?
16. Are impairments described and measured using the AMA
Guides?
QME Form 111 (rev. Mar. 2007)
17. If the AMA Guides are used, are percentages of impairment stated?
18. Are there any relevant diagnostic test results
19.What are the diagnoses? (List) _________________________________________________________________________
_________________________________________________________________________________________________________
20. |
Were medical records reviewed? |
|
|
21. |
Were other physicians consulted? |
Yes |
No |
________________________________________________________________________________________________________
QME
22.Signature:___________________________________________________________Date:__________________________
23.Name:_____________________________________________________Specialty:_______________________________
24.Street Address:______________________________________City:___________________________Zip:_____________
25.Phone:_______________________________________ Cal. License No.:_______________________________________
Declaration of Service of Medical - Legal Report (Lab. Code § 4062.3(i))
I, _______________________________, declare under penalty of perjury under the laws of the State of California that:
(Print Name)
1.I am over the age of 18 and am employed by _________________________________________________________. (Name of Employer)
2.On _____________________________, I served this QME or AME Summary Form with the attached medical- (Date)
legal report on each of the persons/firms named below, and by using the means of service, indicated below. I further declare that I am readily familiar with the practice of this office, named in (1), above, for collection and processing of correspondence for mailing, which is to deposit envelopes with the U.S. Postal Service on that same day with postage fully prepaid thereon at
________________________________,______________ in the ordinary course of business.
(City)(State)
I further declare that for service by mail, I either deposited this document personally in the U.S. Mail, or that I placed it for normal collection with the office stated in (1) above, in time for collection and processing that same day.
For service by messenger delivery: I further declare that I am familiar with the practice of the office stated in (1), above for messenger delivery, and I caused this document to be placed in a sealed envelope and to be delivered to a courier employed by
____________________________________________________ for personal delivery of each such envelope to the addressee,
within two working days, at the address and on the date indicated in below:
Means of service: |
Date: |
Addressee and Address: |
(e.g. U.S. mail/Certified mail/ |
|
|
Overnight mail/ |
|
|
Service by courier) |
|
|
____________________ |
________ |
_________________________________________________ |
____________________ |
________ |
_________________________________________________ |
____________________ |
________ |
_________________________________________________ |
_____________________ |
________ |
_________________________________________________ |
Signed this ______________day of _________________,20_____,in the county of _________________, ___________
|
(State) |
_______________________________________________ |
____________________________________________ |
(Signature of Declarant) |
(Print Name) |
QME Form 111 (rev. Mar. 2007) |
|
Department of Industrial Relations Division of Workers’ Compensation – Medical Unit
PO Box 71010, Oakland, CA 94612 (510)
INSTRUCTIONS
To the QME or AME: You are required by Labor Code section 4062.3(i) to summarize the medical findings from your comprehensive
Employee Information: Fill in the employee's full name, address, telephone number and date of injury.
Event Dates: Complete dates that patient called for an appointment, date of initial examination, date referred for consultation(s), if any, and date report served on all parties. Supplying these dates is a legal requirement.
Disputed Medical Issues and Conclusions: Complete this section by checking appropriate box and stating what page(s) or section of the medical legal report contain the narrative for details. If diagnostic or laboratory tests have been ordered and the results or a medical records request is pending, check that box. If you cannot render opinions because of pending information, please complete and serve the report to comply with the
Basis for Conclusions: Check appropriate box and give page numbers or section where the narrative in the full report is found. For diagnoses, in addition to page numbers, please briefly summarize the diagnoses in lay terms where possible. Also, list the name and specialty for other physicians who provided information used in the medical legal report.
QME Signature: Remember under the Labor Code, all your reports must be signed under the penalty of perjury. You are required to serve the medical legal report and this form on the employee, the claims administrator (if none, the employer) and the Disability Evaluation Unit (DEU) having jurisdiction over the employee's area of residence.
Declaration of Service of Medical – Legal reports: Labor Code sections 139.2(j)(1)(A) and 4062.3 (i) and section 38 of Title 8 of the California Code of Regulations require the QME or AME to serve the
QME Form 111 (rev. Mar. 2007)