
You'll find nothing complicated related to filling out the ca how quarterly status after you open our PDF editor. Following these basic steps, you'll receive the fully filled out PDF document in the shortest time period feasible.
Step 1: To start with, pick the orange "Get form now" button.
Step 2: Right now, you can begin editing your ca how quarterly status. Our multifunctional toolbar is readily available - insert, delete, adjust, highlight, and do other commands with the content in the file.
Get the ca how quarterly status PDF and enter the information for each and every segment:
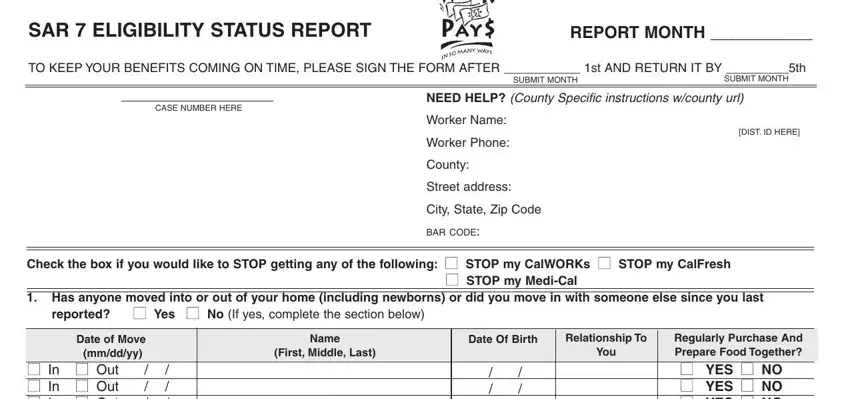
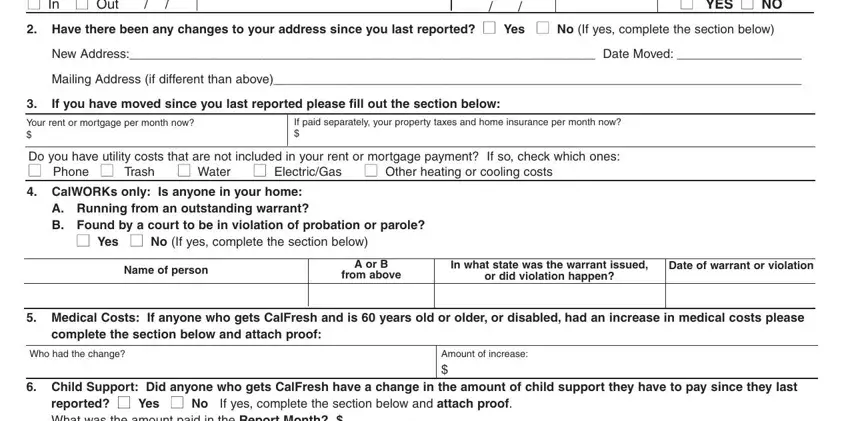
Fill in the Regularly Purchase And Prepare, New Address Date Moved, Mailing Address if different than, If you have moved since you last, Your rent or mortgage per month, If paid separately your property, Do you have utility costs that are, A Running from an outstanding, cid Yes cid No If yes complete the, Name of person, A or B from above, In what state was the warrant, Date of warrant or violation, Medical Costs If anyone who gets, and complete the section below and areas with any content that can be asked by the software.
The software will request you to note particular valuable particulars to easily submit the field reported cid Yes cid No If yes, Dependent Care If anyone who gets, outofpocket dependent care costs, Did anyone Get buy sell trade or, lotterycasino winnings back, If you need more space attach a, Who, Type of Property, When, AmountValue, cid Bought cid Sold cid Gave Away, SAR ELIGIBILITY STATUS REPORT, and PAGE OF.
In the field Did anyone get income from, Job, Job, Name of person who got income, How often paid, Selfemployed check here cid cid, Selfemployed check here cid cid, Selfemployed check here cid cid, Gross amount of income they got in, DATES RECEIVED, DATES RECEIVED, DATES RECEIVED, Hours worked per month Will there, cid Yes cid No If yes explain here, and Did anyone get money from any, write down the rights and obligations of the parties.
Prepare the template by taking a look at these fields: Name, Source of income, One time payment or monthly, How much, Will there be any changes to, CalWORKs only Have any of the, If yes check below and attach, cid Yes cid No, nonCalifornia Domestic Partnership, cid JobEmployment Start stop quit, For Age or older student started, cid Someone paid for all of my, Please read carefully sign and date, By signing this form, and I understand and certify under.
Step 3: As you select the Done button, your ready form can be easily exported to each of your gadgets or to electronic mail given by you.
Step 4: To avoid probable forthcoming complications, be sure to possess a minimum of a couple of duplicates of each and every document.
