

Handling PDF files online is always a piece of cake using our PDF tool. Anyone can fill in usda 3551 21 fillable form here within minutes. The tool is constantly updated by our staff, acquiring useful functions and turning out to be greater. Here is what you will need to do to start:
Step 1: Press the "Get Form" button in the top section of this page to get into our PDF editor.
Step 2: With the help of this state-of-the-art PDF editing tool, it is easy to do more than just fill in blank fields. Edit away and make your documents seem sublime with custom text added in, or modify the original content to excellence - all supported by the capability to incorporate any photos and sign it off.
Completing this PDF calls for attention to detail. Make certain all necessary fields are done properly.
1. While completing the usda 3551 21 fillable form, make certain to include all important blanks within the corresponding section. It will help to hasten the process, allowing your information to be handled fast and appropriately.
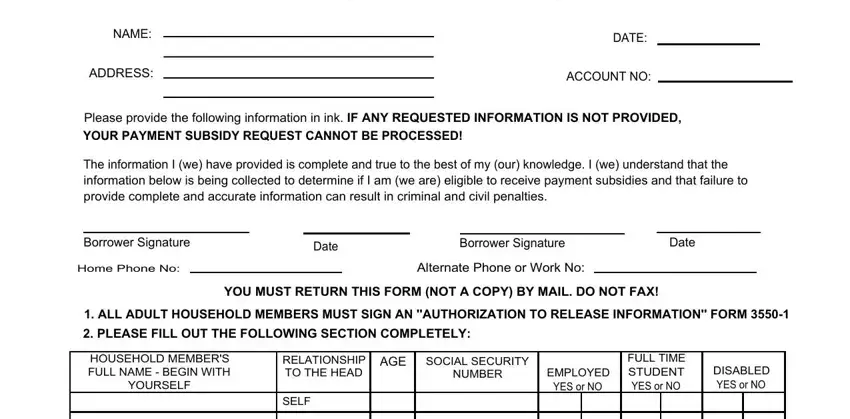
2. Immediately after this section is done, go to type in the relevant information in these - NAME, ADDRESS, PAYMENT SUBSIDY RENEWAL, DATE, ACCOUNT NO, Please provide the following, YOUR PAYMENT SUBSIDY REQUEST, The information I we have provided, Borrower Signature, Home Phone No, Date, Borrower Signature, Date, Alternate Phone or Work No, and YOU MUST RETURN THIS FORM NOT A.
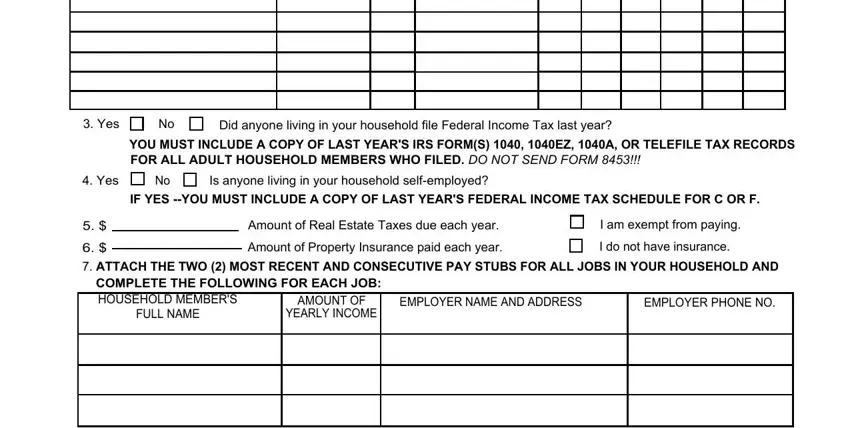
3. Within this part, check out Yes, Did anyone living in your, YOU MUST INCLUDE A COPY OF LAST, Yes, Is anyone living in your household, IF YES YOU MUST INCLUDE A COPY OF, Amount of Real Estate Taxes due, Amount of Property Insurance paid, I am exempt from paying, I do not have insurance, ATTACH THE TWO MOST RECENT AND, COMPLETE THE FOLLOWING FOR EACH, AMOUNT OF, FULL NAME, and YEARLY INCOME. Each of these will need to be taken care of with highest precision.
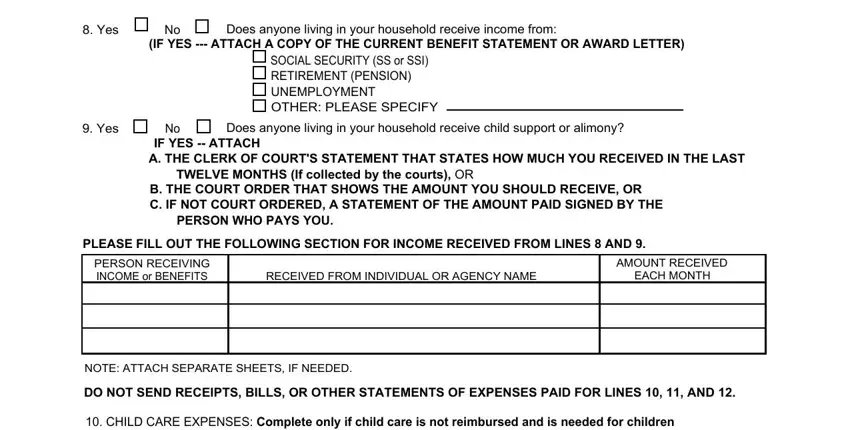
4. All set to fill in the next portion! In this case you'll get all of these Yes, Does anyone living in your, IF YES ATTACH A COPY OF THE, SOCIAL SECURITY SS or SSI, Yes, Does anyone living in your, IF YES ATTACH A THE CLERK OF, TWELVE MONTHS If collected by the, B THE COURT ORDER THAT SHOWS THE, PERSON WHO PAYS YOU, PLEASE FILL OUT THE FOLLOWING, PERSON RECEIVING INCOME or BENEFITS, RECEIVED FROM INDIVIDUAL OR AGENCY, AMOUNT RECEIVED, and EACH MONTH fields to fill in.
5. To wrap up your document, this final segment features several extra blanks. Entering NAME OF CHILD, CARE PROVIDERS OR EDUCATIONAL, PHONE NO, COST PER WEEK, ENABLED TO WORK OR GO TO SCHOOL, Hours, Hours, MEDICAL EXPENSES Complete only if, TYPE OF MEDICAL EXPENSES, TOTAL AMOUNT OF EXPENSE EACH YEAR, DOCTOR, HOSPITAL, MEDICAL INSURANCE, DRUGS or PHARMACEUTICALS, and OTHER Specify will finalize everything and you're going to be done quickly!
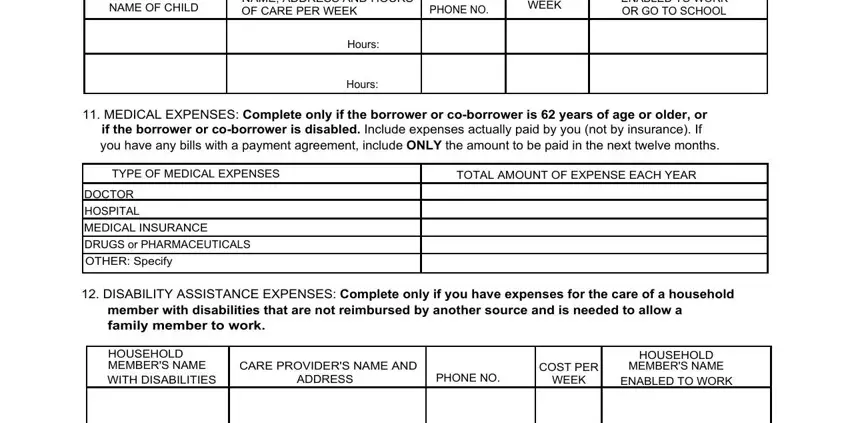
People who use this form generally make some mistakes when filling out Hours in this section. You need to read again everything you type in right here.
Step 3: Check the details you've typed into the form fields and then click the "Done" button. Right after getting afree trial account with us, it will be possible to download usda 3551 21 fillable form or email it directly. The document will also be available through your personal account with your every modification. We don't share the details you use while completing documents at our site.