
You can prepare III effectively in our PDFinity® PDF editor. FormsPal is dedicated to making sure you have the absolute best experience with our editor by continuously introducing new capabilities and improvements. With these improvements, using our tool gets better than ever! If you are looking to get started, this is what it's going to take:
Step 1: Simply hit the "Get Form Button" above on this page to open our pdf editor. There you'll find everything that is required to work with your document.
Step 2: The tool provides you with the opportunity to customize your PDF in a range of ways. Enhance it by writing your own text, correct existing content, and put in a signature - all doable within a few minutes!
It will be an easy task to fill out the document following our detailed guide! Here is what you should do:
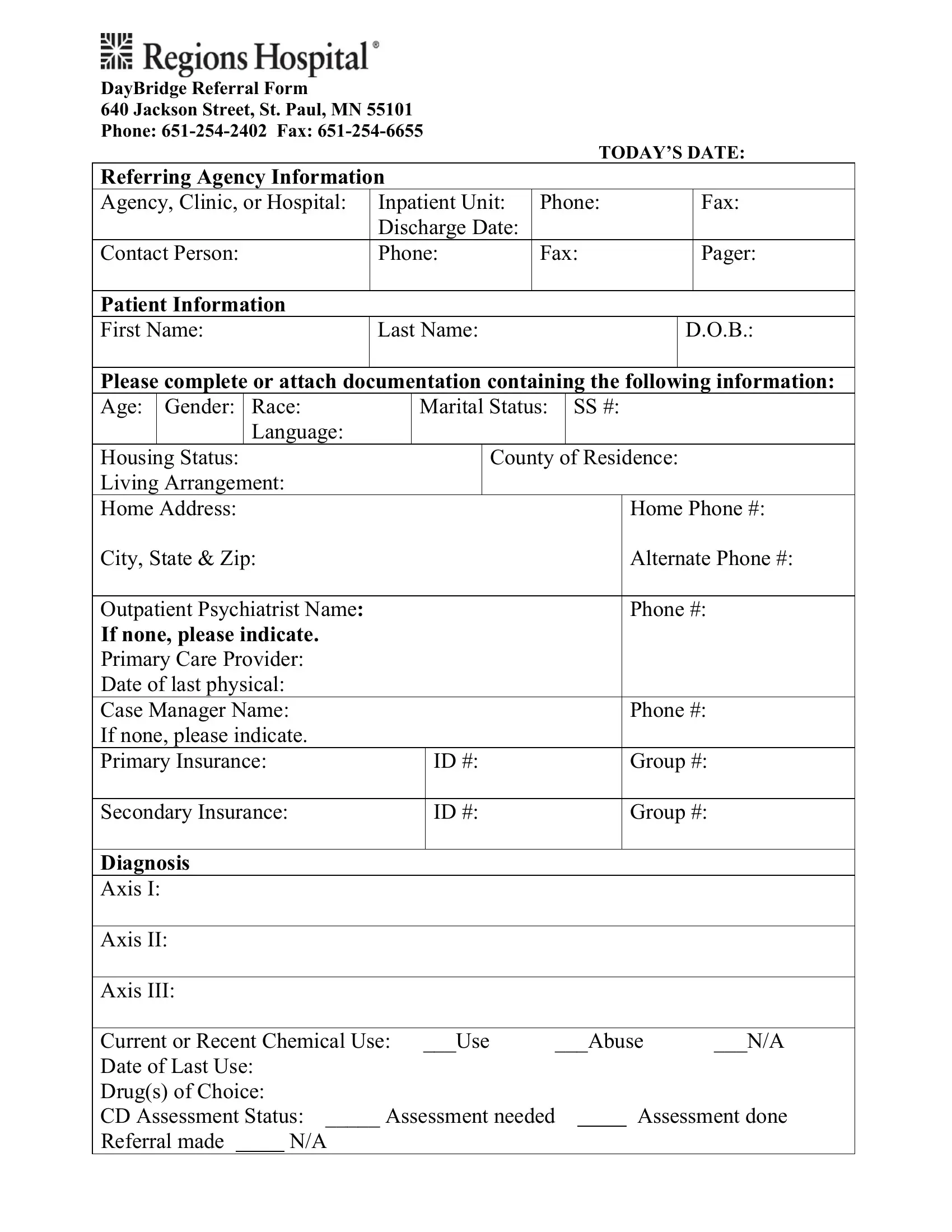
1. Start filling out the III with a group of essential fields. Gather all the required information and ensure absolutely nothing is missed!
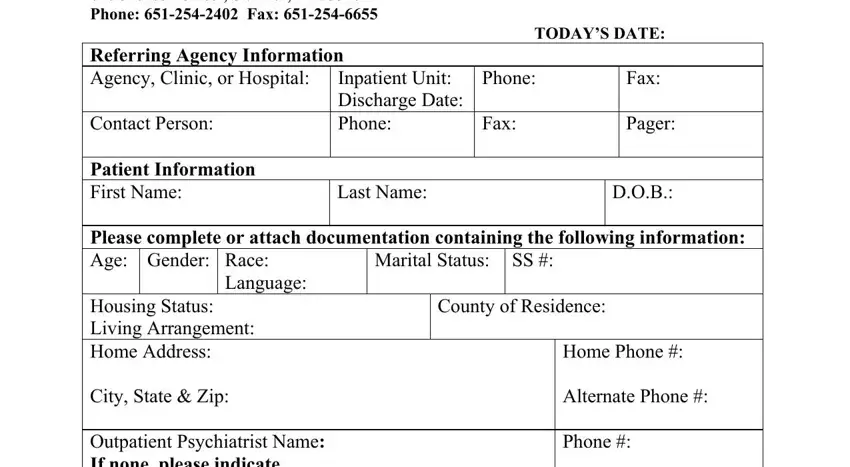
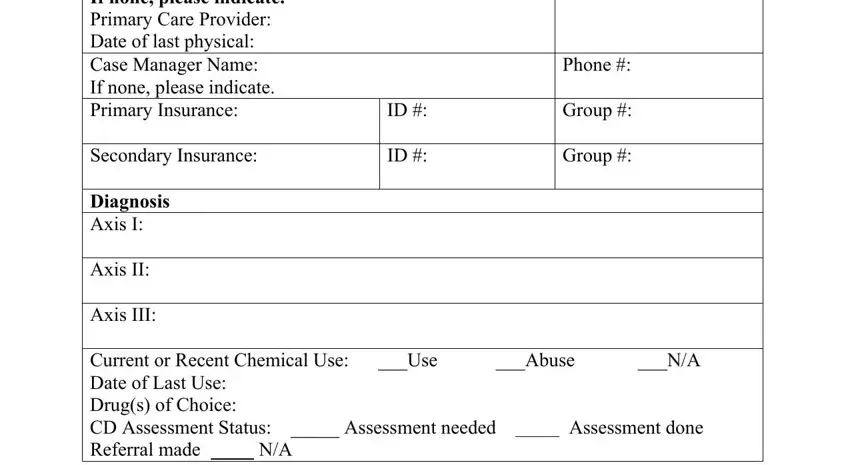
2. Now that the previous segment is done, you'll want to add the necessary specifics in Housing Status Living Arrangement, Secondary Insurance, Home Phone Alternate Phone Phone, Phone, Group Group, and Diagnosis Axis I Axis II Axis III allowing you to progress further.
3. Completing Is Client Dangerous to Self or is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
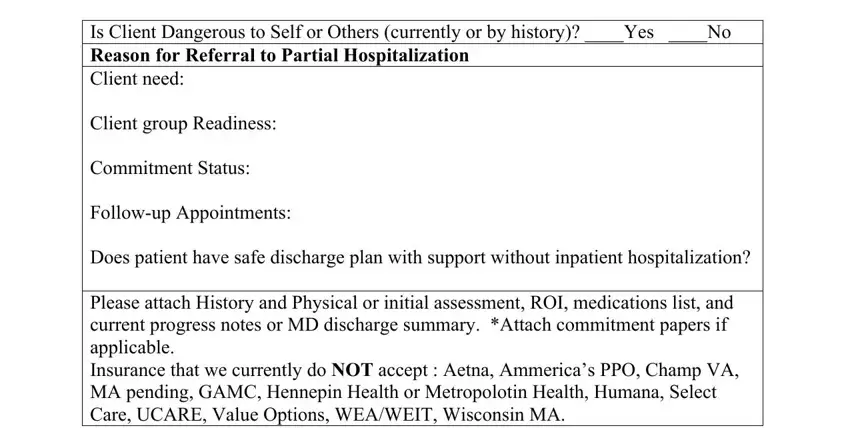
As to Is Client Dangerous to Self or and Is Client Dangerous to Self or, be certain you get them right here. Both of these are considered the key fields in the file.
Step 3: After you have glanced through the details in the blanks, press "Done" to conclude your document generation. Get the III when you sign up for a free trial. Quickly access the document within your personal account, with any modifications and changes automatically kept! We don't sell or share any details you type in while filling out documents at our site.