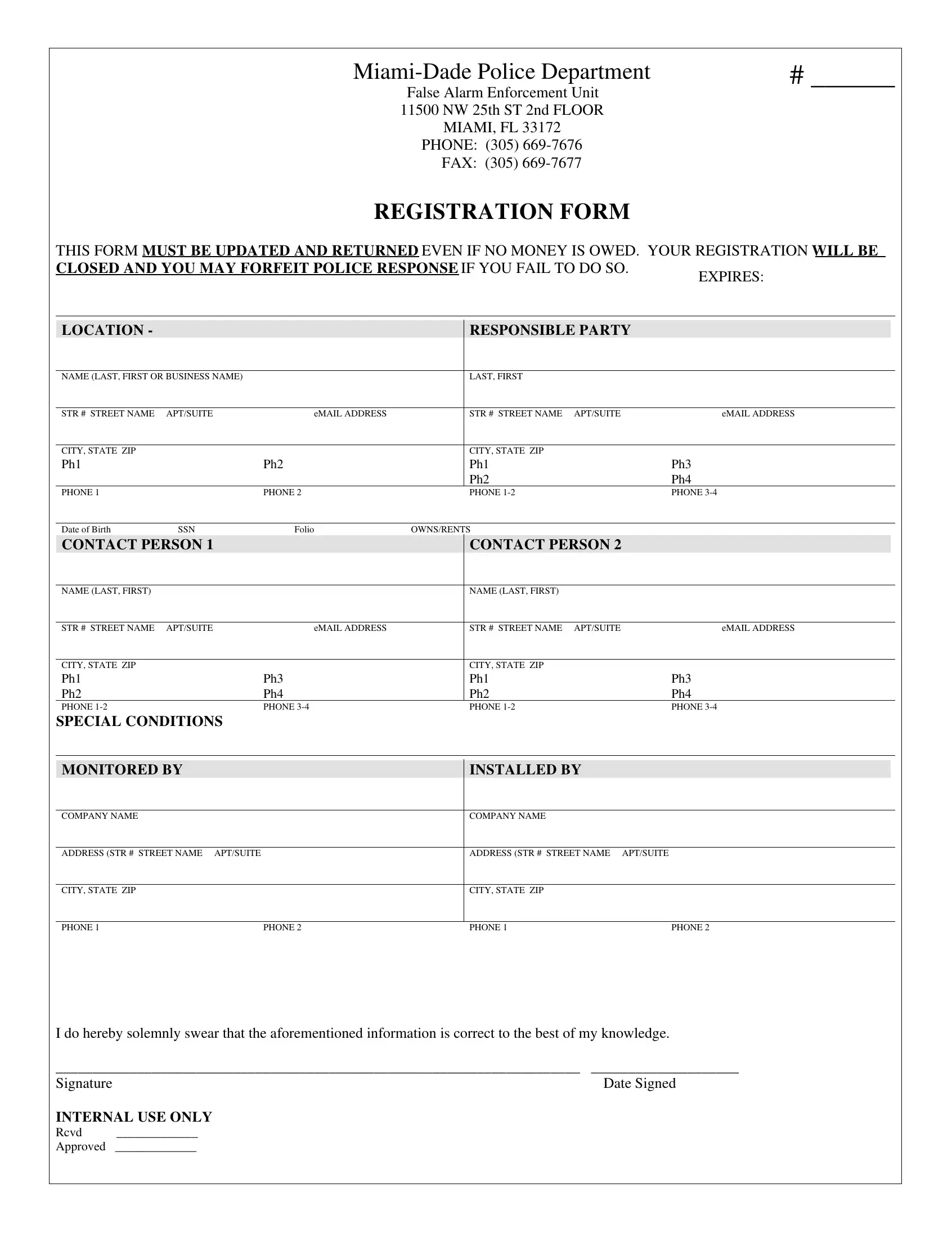
In the heart of Miami, the Miami-Dade Police Department has implemented a crucial administrative process aimed at managing and mitigating the impact of false alarms through the registration Alarm Form. Located at the False Alarm Enforcement Unit’s office, this form is a mandatory requirement for residents and business owners within the jurisdiction. It mandates the timely update and return of the form to ensure continuous registration, failing which could lead to the closure of the registration and the possible forfeiture of police response services in the event of an alarm. The form is comprehensive, requiring detailed information covering location, responsible party details, ownership status, and direct contacts for immediate communication. It also demands specifics about the alarm system in place, including the installation and monitoring agencies. This commitment to accuracy and ongoing communication underscores the department's dedication to keeping both property and occupants safe while also managing departmental resources effectively. Furthermore, by stipulating that the form must be returned even if no moneys are owed, it accentuates the importance of the information over financial obligations, ensuring that all parties are accountable and that the police department can provide an optimal level of service.
| Question | Answer |
|---|---|
| Form Name | Registration Form Alarm |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | miami dade registration form alarm, miami dade alarm permit renewal, miami dade police department alarm permit registration form, miami dade alarm permit |
# ______ |
False Alarm Enforcement Unit 11500 NW 25th ST 2nd FLOOR MIAMI, FL 33172
PHONE: (305)
REGISTRATION FORM
THIS FORM MUST BE UPDATED AND RETURNED EVEN IF NO MONEY IS OWED. YOUR REGISTRATION WILL BE
CLOSED AND YOU MAY FORFEIT POLICE RESPONSE IF YOU FAIL TO DO SO.
EXPIRES:
LOCATION - |
|
|
|
RESPONSIBLE PARTY |
|
|
|
|
|
|
|
|
|
|
|
NAME (LAST, FIRST OR BUSINESS NAME) |
|
|
LAST, FIRST |
|
|
|
|
|
|
|
|
|
|
|
|
STR # STREET NAME |
APT/SUITE |
eMAIL ADDRESS |
|
STR # STREET NAME |
APT/SUITE |
eMAIL ADDRESS |
|
|
|
|
|
|
|
|
|
CITY, STATE ZIP |
|
|
|
CITY, STATE ZIP |
|
|
|
Ph1 |
|
Ph2 |
|
Ph1 |
|
Ph3 |
|
|
|
|
|
Ph2 |
|
Ph4 |
|
PHONE 1 |
|
PHONE 2 |
|
PHONE |
|
PHONE |
|
|
|
|
|
|
|
|
|
Date of Birth |
SSN |
Folio |
OWNS/RENTS |
|
|
|
|
CONTACT PERSON 1 |
|
|
CONTACT PERSON 2 |
|
|
||
|
|
|
|
|
|
|
|
NAME (LAST, FIRST) |
|
|
|
NAME (LAST, FIRST) |
|
|
|
|
|
|
|
|
|
|
|
STR # STREET NAME |
APT/SUITE |
eMAIL ADDRESS |
|
STR # STREET NAME |
APT/SUITE |
eMAIL ADDRESS |
|
|
|
|
|
|
|
|
|
CITY, STATE ZIP |
|
|
|
CITY, STATE ZIP |
|
|
|
Ph1 |
|
Ph3 |
|
Ph1 |
|
Ph3 |
|
Ph2 |
|
Ph4 |
|
Ph2 |
|
Ph4 |
|
PHONE |
|
PHONE |
|
PHONE |
|
PHONE |
|
SPECIAL CONDITIONS
MONITORED BY
INSTALLED BY
COMPANY NAME
COMPANY NAME
ADDRESS (STR # STREET NAME APT/SUITE
ADDRESS (STR # STREET NAME APT/SUITE
CITY, STATE ZIP
CITY, STATE ZIP
PHONE 1 |
PHONE 2 |
PHONE 1 |
PHONE 2 |
I do hereby solemnly swear that the aforementioned information is correct to the best of my knowledge.
_______________________________________________________________________ |
____________________ |
Signature |
Date Signed |
INTERNAL USE ONLY |
|
Rcvd _____________
Approved _____________