

Using PDF forms online can be super easy with this PDF editor. Anyone can fill in certificate fetal death of here within minutes. Our team is dedicated to providing you with the ideal experience with our editor by constantly adding new capabilities and upgrades. With these updates, working with our tool becomes easier than ever before! Here is what you would need to do to start:
Step 1: Click on the orange "Get Form" button above. It'll open our pdf tool so that you can start filling in your form.
Step 2: With this state-of-the-art PDF editing tool, you can do more than just complete blank form fields. Edit away and make your docs appear great with custom textual content added, or adjust the file's original content to excellence - all that comes with the capability to incorporate your personal pictures and sign it off.
This form will need some specific details; to ensure accuracy, please be sure to adhere to the tips further on:
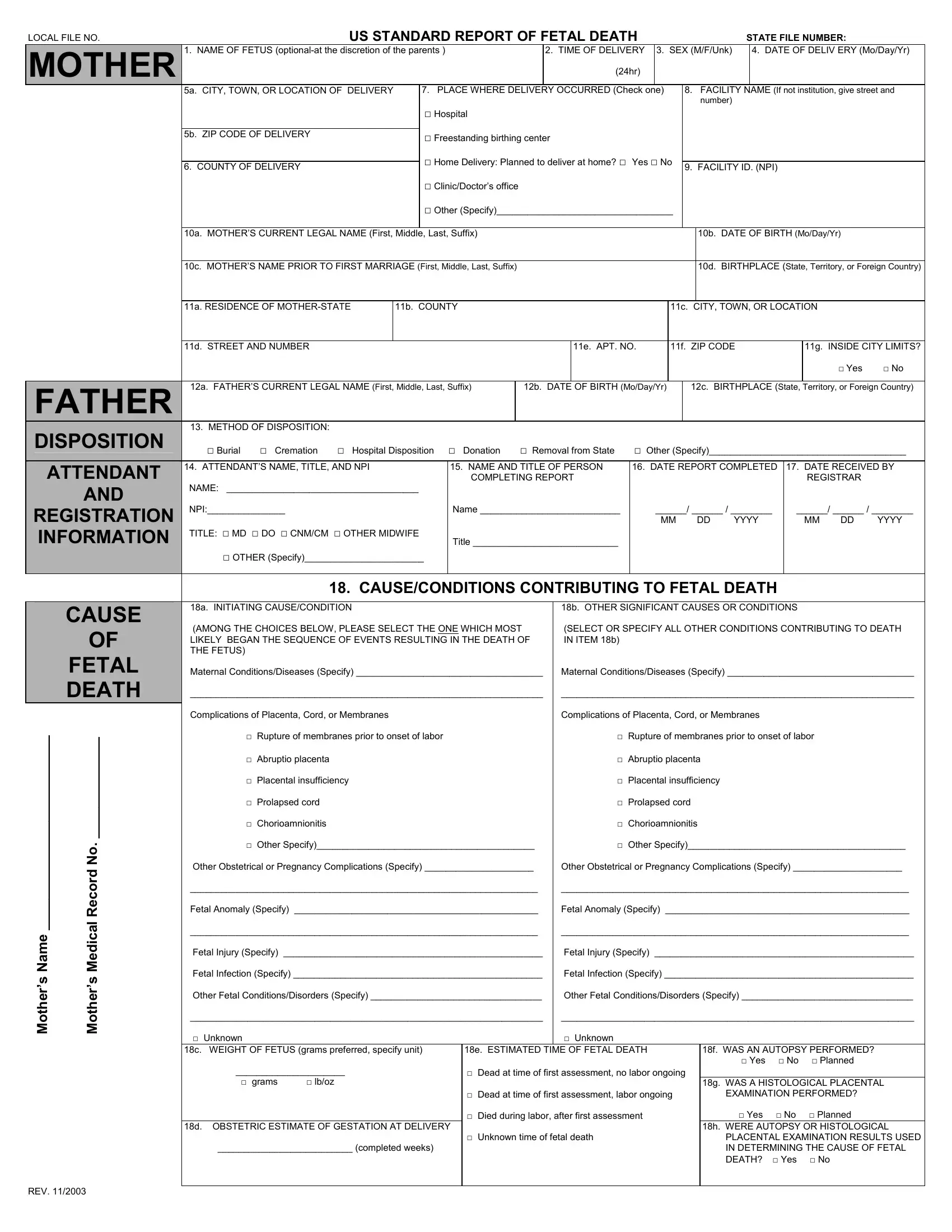
1. Begin completing the certificate fetal death of with a group of essential fields. Gather all of the required information and make certain nothing is missed!
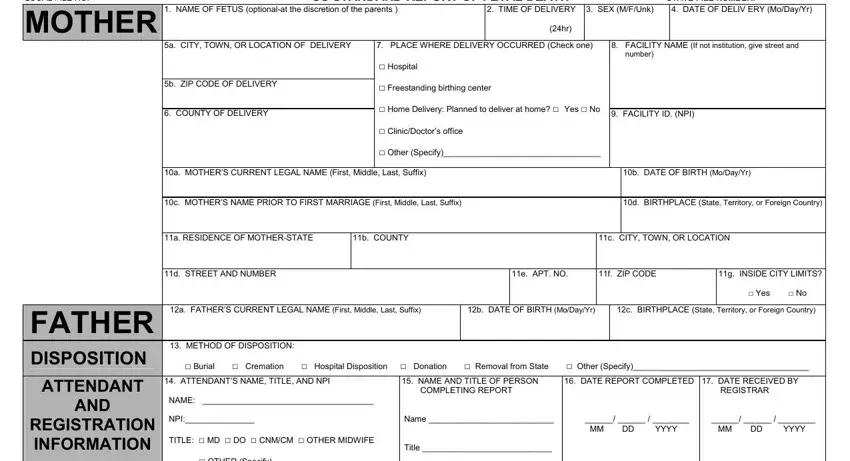
2. Once your current task is complete, take the next step – fill out all of these fields - FETAL DEATH, o N d r o c e R, l a c i d e M s r e h t o M, e m a N s, Chorioamnionitis, Abruptio placenta, Rupture of membranes prior to, Prolapsed cord, Placental insufficiency, a INITIATING CAUSECONDITION AMONG, Other Specify, d OBSTETRIC ESTIMATE OF GESTATION, Abruptio placenta, Rupture of membranes prior to, and Prolapsed cord with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
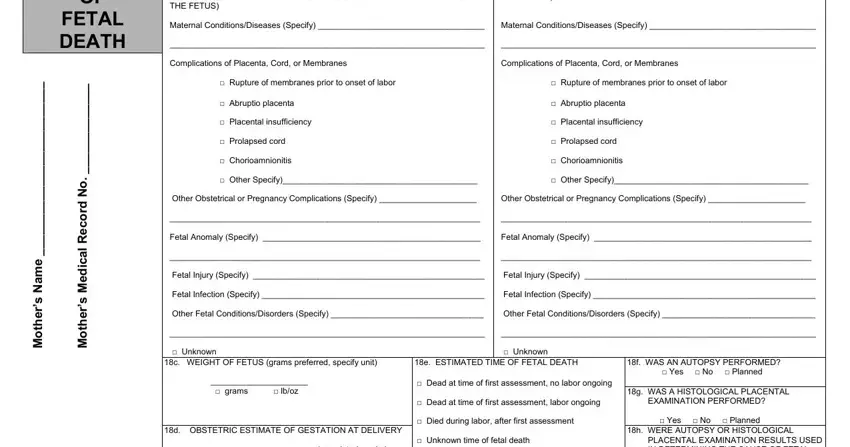
Regarding FETAL DEATH and Rupture of membranes prior to, be sure you double-check them in this section. Both of these are considered the key ones in this file.
3. The following segment is mostly about REV, d OBSTETRIC ESTIMATE OF GESTATION, and f WAS AN AUTOPSY PERFORMED Yes - fill in all these blanks.

4. The form's fourth subsection arrives with these particular fields to focus on: MOTHER, MEDICAL, MOTHER OF HISPANIC ORIGIN Check, MOTHERS EDUCATION Check the box, MOTHERS RACE Check one or more, a DATE OF FIRST PRENATAL CARE, b DATE OF LAST PRENATAL CARE VISIT, TOTAL NUMBER OF PRENATAL VISITS, MOTHERS PREPREGNANCY WEIGHT, MOTHERS WEIGHT AT DELIVERY pounds, DID MOTHER GET WIC FOOD FOR, NUMBER OF OTHER PREGNANCY, CIGARETTE SMOKING BEFORE AND, DATE LAST NORMAL MENSES BEGAN, and PLURALITY Single Twin Triplet.
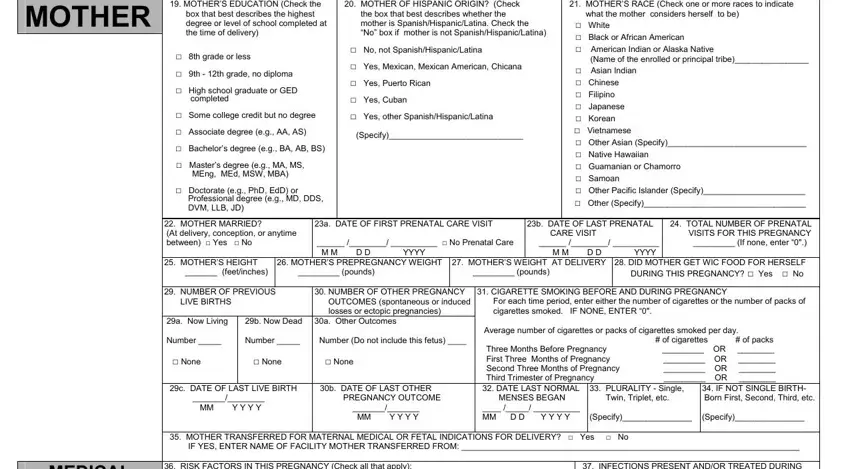
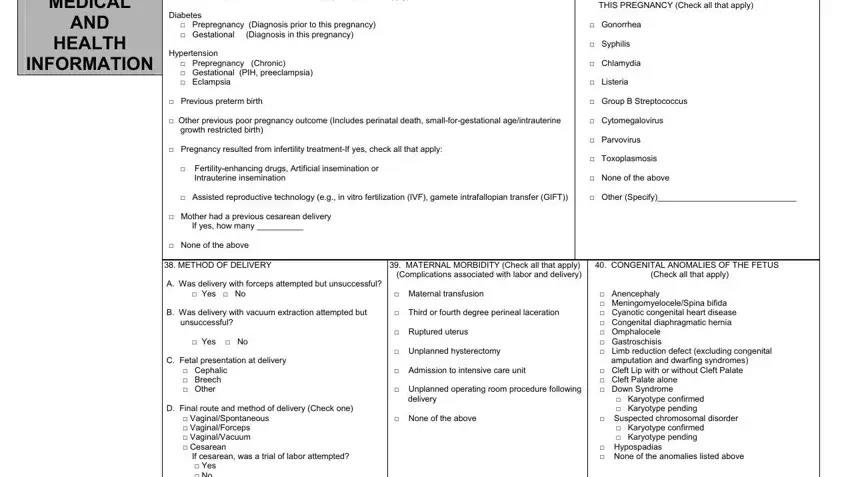
5. This form has to be concluded within this area. Below you will notice a comprehensive listing of fields that require appropriate details for your document usage to be accomplished: MEDICAL, AND, HEALTH, INFORMATION, RISK FACTORS IN THIS PREGNANCY, MATERNAL MORBIDITY Check all that, INFECTIONS PRESENT ANDOR TREATED, and CONGENITAL ANOMALIES OF THE FETUS.
Step 3: After you have looked over the information in the file's blank fields, click "Done" to conclude your form at FormsPal. Create a 7-day free trial plan at FormsPal and acquire immediate access to certificate fetal death of - which you'll be able to then work with as you wish in your personal account page. FormsPal guarantees your data confidentiality by having a secure method that in no way records or shares any sort of personal information used in the form. Rest assured knowing your files are kept protected each time you use our editor!