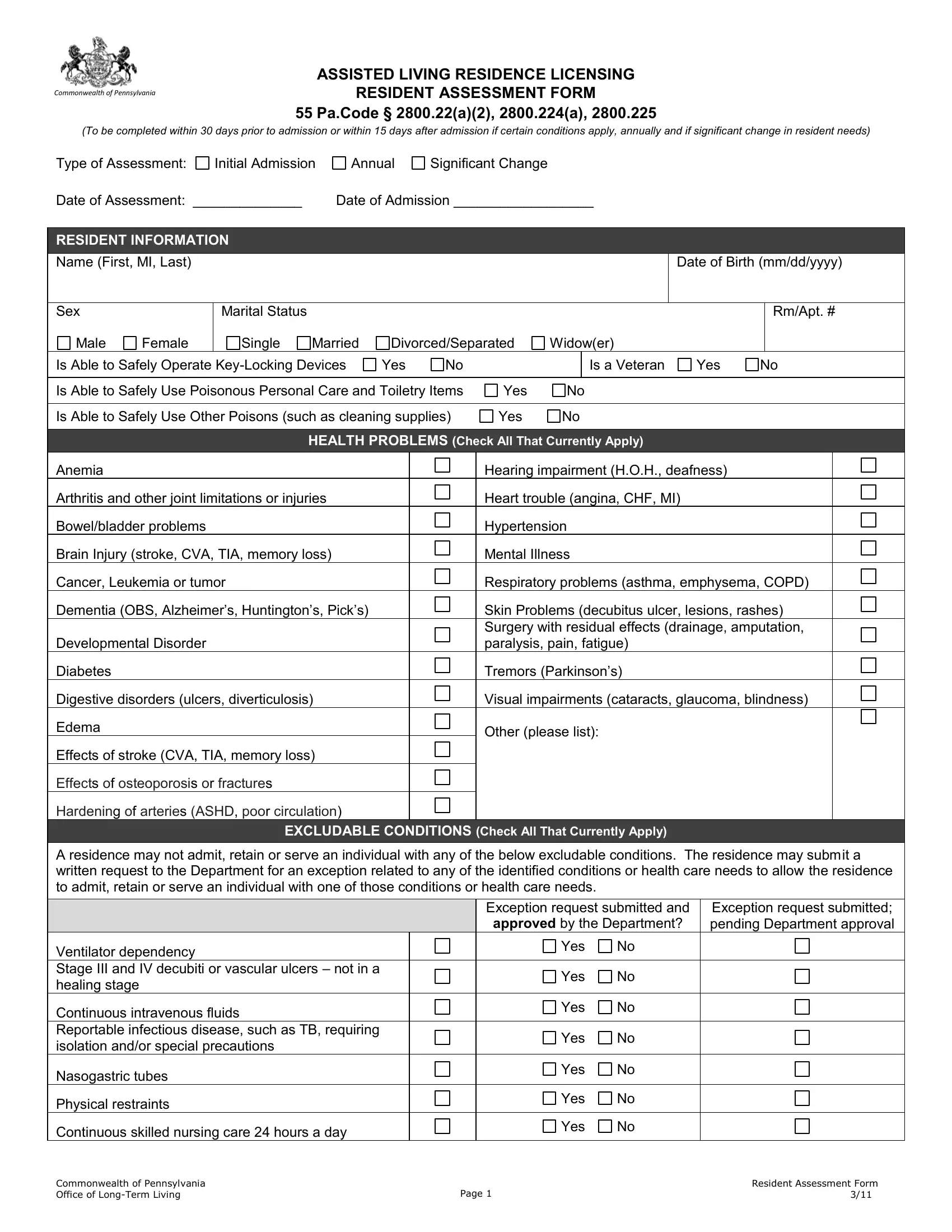
Preparing for a person's entry into an assisted living residence requires meticulous planning and understanding of their needs and capabilities to ensure they receive the appropriate level of support. The Resident Assessment Form used by the Commonwealth of Pennsylvania is a comprehensive instrument designed to capture crucial information within various domains such as personal information, health problems, medications, mobility, emergency evacuation needs, personal care needs, dietary preferences, healthcare management, housekeeping abilities, miscellaneous daily living tasks, communication capabilities, and behavioral or cognitive conditions. This form must be completed either within 30 days prior to admission or within 15 days following admission, and it is also required annually or in the event of a significant change in the resident's needs. Such thorough assessments guide the formulation of individualized care plans, ensuring each resident's health, safety, and well-being are proactively managed. Additionally, the form looks into preferences and interests, thereby personalizing the care and enhancing the quality of life in the assisted living setting. Furthermore, it outlines specific excludable conditions that may necessitate additional approval from the Department of Health to ensure the facility can adequately meet the needs of those requiring more intensive support.
| Question | Answer |
|---|---|
| Form Name | Resident Assessment Form |
| Form Length | 8 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 2 min |
| Other names | pennsylvania residence resident assessment form, TIA, COPD, selfadministration |
