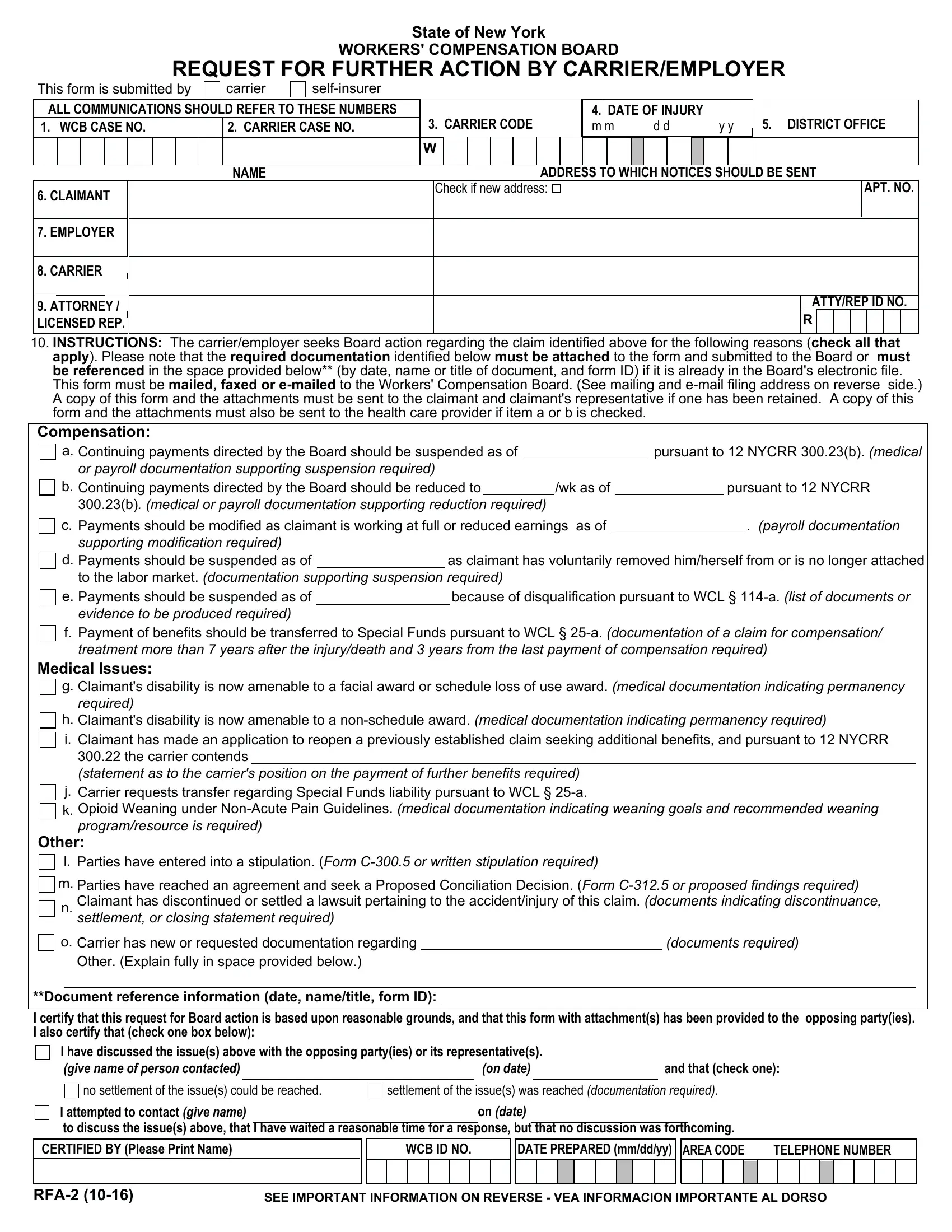
TO THE CARRIER/EMPLOYER
This form may be filed by the insurance carrier or employer in a workers' compensation case when it wants the Workers' Compensation Board to take action in the case. ATTACH ALL APPLICABLE EVIDENCE FOR CONSIDERATION BY THE BOARD. A copy of this form and the attachments must also be sent to the claimant, and his/her representative, if any. ITEMS a and b replace Form C-22b. If item a or b is checked, a copy of this form and the attachments must also be filed with claimant's attending doctor. If you would like on-line access to the case, you can register for eCase using the registration instructions available on the Board website under the eCase link.
Regarding Items a and b - Board Rule 12 NYCRR 300.23
This notice (items a and b) replaces Form C-22b for the purpose of notifying the Board of the carrier/employer's intention to reduce or suspend the claimant's payments in accordance with Board Rule 12 NYCRR 300.23. This notice may be filed in any case where there has been an award and a direction for continuation of payments and evidence is presented to support the suspension of payments or reduction in rate.
The Board, upon receipt of this notice and attachments, may either schedule a WC LAW JUDGE HEARING on this issue within 20 days during any period in which regular hearings are scheduled, or refer the matter to the Administrative Review Division for a determination of whether a reopening is warranted. In the event that the Administrative Review Division directs that the case be reopened, a WC Law Judge Hearing will be scheduled in an expeditious manner. IF THE REQUIRED DOCUMENTATION IS NOT ATTACHED, THE CASE WILL NOT BE SCHEDULED FOR A HEARING.
Cases at hearing points which do not have regularly scheduled hearings within 20 days may be scheduled at another hearing point. At the time a WC Law Judge hearing is held, either immediately after the Board's receipt of this notice and attachments or at the direction of the Administrative Review Division, the WC Law Judge will consider all available evidence and decide whether or not payments may be suspended or reduced.
PAYMENTS SHALL CONTINUE, AS DIRECTED, until there is a determination by the WC Law Judge that such payments may be suspended or reduced.
TO THE CLAIMANT
If you have any questions regarding the action being requested by the carrier/employer, please contact the nearest office of the Board. If you have retained legal counsel to represent you, you may contact him/her for assistance. Please remember to always use the WCB Case Number shown on the other side of this form when corresponding with the Board. If you would like to follow your claim on-line, you can register for eCase using the registration instructions available on the Board website under the eCase link.
AL RECLAMANTE
Si tiene alguna pregunta en relación a la acción solicitada por el patrono ó el seguro favor de comunicarse con la oficina más cercana de la Junta. Si está representado legalmente, debe comunicarse con sú representante para asesoramiento. Cuando se comunique con la Junta, siempre use el número de caso WCB que aparece en el otro lado de esta notificación. Si desea realizar un seguimiento en línea de su reclamo, puede registrarse para ingresar a eCase utilizando las instrucciones para registro que están disponibles en el sitio web de la WCB en el enlace eCase.
TO THE CLAIMANT - Regarding Items a and b
Please read this notice and attachments carefully. If item a or b is checked, this notice means that your employer (if self-insured) or its insurance company wants to suspend or reduce your compensation payments, for the reason indicated.
As explained above, your case may be scheduled for a hearing on this issue. Be sure to BE PRESENT, if you disagree with your employer or his/her insurance company. If you are NOT PRESENT, the W.C. Law Judge will make a decision based on available evidence. If your employer or his/her insurance company contends that your compensation payments should be suspended or reduced because your medical condition has improved (not because your earnings have increased), BRING TO YOUR HEARING THE MOST RECENT MEDICAL REPORT FROM YOUR DOCTOR THAT DESCRIBES YOUR CURRENT MEDICAL CONDITION.
PARA EL RECLAMANTE - Respecto de los puntos a y b
Lea atentamente esta notificación y los documentos adjuntos. Si están marcados los puntos a o b, esta notificación significa que el empleador (en caso de estar auto asegurado) o su compañía aseguradora, desea suspender o reducir los pagos de su indemnización, por el motivo que se indica.
Tal como se explica anteriormente, es posible que se fije una fecha para una audiencia sobre su caso en relación a este asunto. Asegúrese de ESTAR PRESENTE, en caso de que usted esté en desacuerdo con su empleador o su compañía aseguradora. Si usted NO ESTÁ PRESENTE, el juez que dirime sobre cuestiones laborales tomará una decisión a partir de la evidencia disponible. En caso
de que su empleador o su compañía aseguradora aleguen que se deben suspender o reducir los pagos de su indemnización debido a una mejoría de su condición médica (no debido a un aumento de sus ingresos), PRESENTE EN LA AUDIENCIA EL INFORME
MÉDICO MÁS RECIENTE QUE DESCRIBA SU CONDICIÓN MÉDICA ACTUAL, ESCRITO POR SU MÉDICO.
Section 114 of the Workers' Compensation Law provides, in part, that any employer or carrier, or any employee, agent, or person acting on behalf of an employer or carrier, who knowingly makes a false statement or representation as to a material fact for the purpose of avoiding provision of any payment or benefit under this chapter shall be guilty of a felony.
PO Box 5205
Binghamton, NY 13902-5205
Address for Email Filing: wcbclaimsfiling@wcb.ny.gov
Statewide Fax Line: 877-533-0337
www.wcb.ny.gov