In the evolving landscape of radiology and nuclear medicine, the importance of maintaining rigorous standards for authorized users cannot be overstated. Among the raft of documentation and regulatory compliance requirements, the RHB Form 313A (CE) emerges as a critical tool in the California Department of Public Health's armory. Issued in July 2010, this document serves a dual purpose: it is both a testament to the completion of required refresher training and an attestation by a preceptor on a candidate's readiness to handle radioactive materials for a range of medical applications, including but not limited to uptake, dilution, excretion studies, imaging, and localization studies, as well as the use of unsealed byproduct material across a variety of clinical uses under specific sections of the 10 CFR 35. The form meticulously outlines the prerequisites for individuals seeking authorization or continuation of their status as authorized users. It encapsulates the essence of comprehensive training and hands-on experience in the field, requiring detailed documentation of continuing education, prior authorization, board certification, and clinical training experience accumulated over recent years. Moreover, it emphasizes the relationship between the aspiring authorized user and their preceptor, who plays a pivotal role in validating the candidate's competence and readiness to perform independently in a highly specialized and sensitive medical field.
| Question | Answer |
|---|---|
| Form Name | Rhb Form 313A Ce |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | RHB RML 313A(CE) rhb313a form |
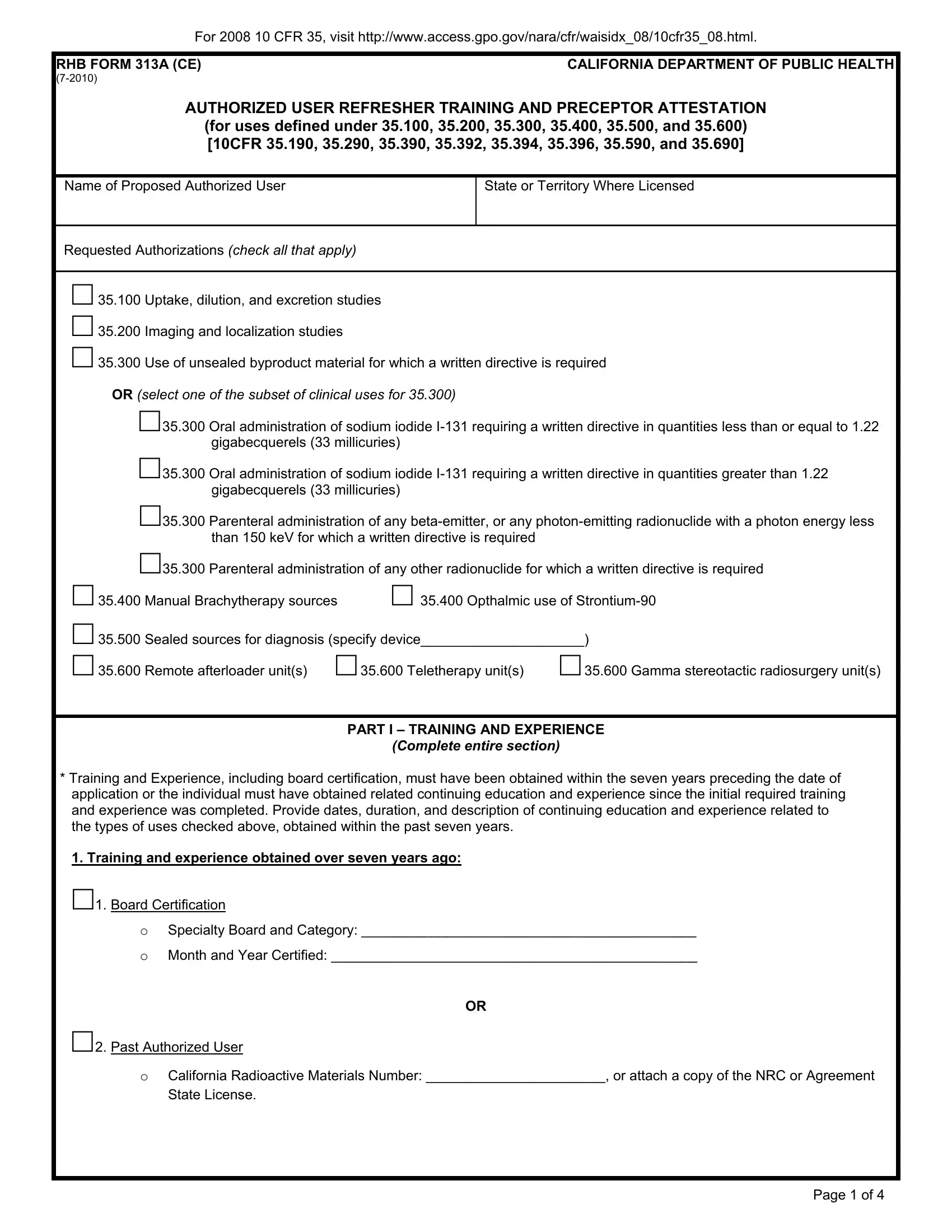
For 2008 10 CFR 35, visit http://www.access.gpo.gov/nara/cfr/waisidx_08/10cfr35_08.html.
RHB FORM 313A (CE) |
CALIFORNIA DEPARTMENT OF PUBLIC HEALTH |
AUTHORIZED USER REFRESHER TRAINING AND PRECEPTOR ATTESTATION (for uses defined under 35.100, 35.200, 35.300, 35.400, 35.500, and 35.600) [10CFR 35.190, 35.290, 35.390, 35.392, 35.394, 35.396, 35.590, and 35.690]
Name of Proposed Authorized User
State or Territory Where Licensed
Requested Authorizations (check all that apply)
□35.100 Uptake, dilution, and excretion studies
□35.200 Imaging and localization studies
□35.300 Use of unsealed byproduct material for which a written directive is required OR (select one of the subset of clinical uses for 35.300)
□35.300 Oral administration of sodium iodide
□35.300 Oral administration of sodium iodide
□35.300 Parenteral administration of any
□35.300 Parenteral administration of any other radionuclide for which a written directive is required
□35.400 Manual Brachytherapy sources □ 35.400 Opthalmic use of
□ 35.500 |
Sealed sources for diagnosis (specify device_____________________) |
||
□ 35.600 |
Remote afterloader unit(s) |
□35.600 Teletherapy unit(s) |
□35.600 Gamma stereotactic radiosurgery unit(s) |
PART I – TRAINING AND EXPERIENCE
(Complete entire section)
*Training and Experience, including board certification, must have been obtained within the seven years preceding the date of application or the individual must have obtained related continuing education and experience since the initial required training and experience was completed. Provide dates, duration, and description of continuing education and experience related to the types of uses checked above, obtained within the past seven years.
1. Training and experience obtained over seven years ago:
□1. Board Certification
OSpecialty Board and Category: ___________________________________________
OMonth and Year Certified: _______________________________________________
OR
□2. Past Authorized User
OCalifornia Radioactive Materials Number: _______________________, or attach a copy of the NRC or Agreement State License.
Page 1 of 4
For 2008 10 CFR 35, visit http://www.access.gpo.gov/nara/cfr/waisidx_08/10cfr35_08.html.
RHB FORM 313A (CE) |
CALIFORNIA DEPARTMENT OF PUBLIC HEALTH |
CONTINUING EDUCATION AND EXPERIENCE AND PRECEPTOR ATTESTATION (continued)
2. Continuing education and experience within the past seven years:
|
|
|
|
Type and Length of Training |
|||
|
|
|
|
LECTURE/ |
|
SUPERVISED |
|
|
|
|
|
LABORATORY |
LABORATORY |
||
|
|
|
|
COURSES |
|
EXPERIENCE |
|
FIELD OF TRAINING |
LOCATION AND DATES OF TRAINING |
(HOURS) |
|
(HOURS) |
|||
A |
|
B |
C |
|
D |
||
a. Radiation physics and instrumentation |
|
|
|
|
|
|
|
b. Radiation protection |
|
|
|
|
|
|
|
c. Mathematics pertaining to use and |
|
|
|
|
|
|
|
measurement of radioactivity |
|
|
|
|
|
|
|
d. Chemistry of byproduct material for |
|
|
|
|
|
|
|
medical use (not required for 35.590) |
|
|
|
|
|
|
|
e. Radiation biology |
|
|
|
|
|
|
|
4. Clinical Training and Experience (Use back if more space is needed) |
|
|
|
|
|||
For 35.300 or any subset of clinical uses under 35.300, complete this section. For all others, skip to page 3. |
|
|
|||||
|
Number of Cases |
|
Location of Experience/License |
|
|
|
|
Description of Experience |
Involving Personal |
|
|
Dates of Experience* |
|||
|
or Permit Number of Facility |
|
|||||
|
Participation |
|
|
|
|
||
|
|
|
|
|
|
|
|
Oral administration of sodium iodide I- |
|
|
|
|
|
|
|
131 requiring a written directive in |
|
|
|
|
|
|
|
quantities less than or equal to 1.22 |
|
|
|
|
|
|
|
gigabecquerels (33 millicuries) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Oral administration of sodium iodide I- |
|
|
|
|
|
|
|
131 requiring a written directive in |
|
|
|
|
|
|
|
quantities greater than 1.22 |
|
|
|
|
|
|
|
gigabecquerels (33 millicuries) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Parenteral administration of any beta- |
|
|
|
|
|
|
|
emitter, or |
|
|
|
|
|
|
|
with a photon energy less than 150 keV |
|
|
|
|
|
|
|
for which a written directive is required |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Parenteral administration of any other |
|
|
|
|
|
|
|
radionuclide for which a written directive |
|
|
|
|
|
|
|
is required |
|
|
|
|
|
|
|
(List radionuclides) |
|
|
|
|
|
|
|
Supervising Individual |
|
|
License/Permit Number listing supervising individual as an |
||||
|
|
|
authorized user (if not listed on a California Radioactive Materials |
||||
|
|
|
License, attach a copy of NRC or Agreement State license) |
||||
|
|
|
|||||
Supervisor meets the requirements below, or equivalent Agreement State requirements (check all that apply)**. |
|
||||||
□ 35.390 |
|
|
With experience administering dosages of: |
|
|||
|
|
Oral |
|||||
□ 35.392 |
|
|
□than or equal to 1.22 gigabecquerels (33 millicuries) |
||||
|
|
|
|
|
|
|
|
□ 35.394 |
|
|
Oral |
||||
|
|
□gigabecquerels (33 millicuries) |
|
|
|||
□ 35.396 |
|
|
Parenteral administration of |
||||
|
|
□emitting radionuclide with a photon energy less than 150 |
|||||
|
|
|
keV requiring a written directive |
|
|
||
|
|
|
Parenteral administration of any other radionuclide |
||||
|
|
|
□requiring a written directive |
|
|
||
**Supervising Authorized User must have experience in administering dosages in the same dosage category or categories as the individual requesting authorized user status.
Page 2 of 4
For 2008 10 CFR 35, visit http://www.access.gpo.gov/nara/cfr/waisidx_08/10cfr35_08.html.
RHB FORM 313A (CE) |
CALIFORNIA DEPARTMENT OF PUBLIC HEALTH |
CONTINUING EDUCATION AND EXPERIENCE AND PRECEPTOR ATTESTATION (continued)
KEY TO COLUMN
a.Supervised examination of patients to determine the suitability for radionuclide diagnosis and/or treatment and recommendation for prescribed dosage.
b.Dose calibration and actual administration of dose to the patient including calculation of the radiation dose and related measurements.
c.Supervised interpretation of results of diagnostic studies.
d.Adequate period of training to enable physician to manage radioactive patients and follow patients through diagnosis and therapy.
ISOTOPE
A
CONDITIONS DIAGNOSED OR
TREATED
B
NUMBER OF
CASES
INVOLVING
PERSONAL
PARTICIPATION
C
COMMENTS
(Additional information or comments may be submitted in duplicate on separate sheets)
D
Complete Part II Preceptor Attestation.
PART II – PRECEPTOR ATTESTATION
Note: This part must be completed by the individual's preceptor. The preceptor does not have to be the supervising individual as long as the preceptor provides, directs, or verifies training and experience required. If more than one preceptor is necessary to document experience, obtain a separate preceptor statement from each.
By checking the boxes below, the preceptor is attesting that the individual has knowledge to fulfill the duties of the position sought and not attesting to the individual's "general clinical competency."
First Section
□I attest that __________________________________ has satisfactorily completed the training and experience
Name of Proposed Authorized User
documented in this form and has achieved a level of competency sufficient to function independently as an authorized user for the medical uses requested above.
Page 3 of 4
For 2008 10 CFR 35, visit http://www.access.gpo.gov/nara/cfr/waisidx_08/10cfr35_08.html.
RHB FORM 313A (CE) |
CALIFORNIA DEPARTMENT OF PUBLIC HEALTH |
CONTINUING EDUCATION AND EXPERIENCE AND PRECEPTOR ATTESTATION (continued)
Second Section (required for 35.390, 35.392, 35.394, and 35.396 only)
Complete and continue to Third Section
□I attest that __________________________________ has satisfactorily completed the required clinical case
Name of Proposed Authorized User
experience required in 35.390(b)(1)(ii)(G) listed below, and has satisfactorily achieved a level of competency to function independently as an authorized user for:
□Oral
□Oral
□Parenteral administration of
□Parenteral administration of any other radionuclide requiring a written directive
Third Section
Complete the following for preceptor attestation and signature:
□I meet the requirements below, or equivalent Agreement State requirements, as an authorized user for:
□ 35.190 |
□ 35.290 |
□ 35.390 |
□ 35.390+ generator experience |
□ 35.392 |
□ 35.394 |
□ 35.396 |
|
Complete the following for 35.390, 35.392, 35.394, and 35.396.
□I have experience administering dosages in the following categories for which the proposed Authorized User is requesting authorization.
□Oral
□Oral
□Parenteral administration of
□Parenteral administration of any other radionuclide requiring a written directive
Name of Preceptor
Signature
Telephone Number
Date
License/Permit Number and Facility Name (if not a California Radioactive Materials License, attach a copy of NRC or Agreement State license)
Page 4 of 4