
Should you intend to fill out ri school physical, you won't have to install any applications - simply use our PDF editor. Our tool is consistently evolving to give the very best user experience achievable, and that's because of our commitment to continuous development and listening closely to feedback from users. To get the ball rolling, take these basic steps:
Step 1: Access the PDF in our editor by clicking the "Get Form Button" in the top section of this webpage.
Step 2: With our handy PDF editing tool, you'll be able to accomplish more than just complete blanks. Edit away and make your forms appear perfect with customized textual content incorporated, or modify the original input to excellence - all comes along with the capability to incorporate almost any photos and sign the document off.
It is actually straightforward to finish the pdf using this practical guide! Here's what you want to do:
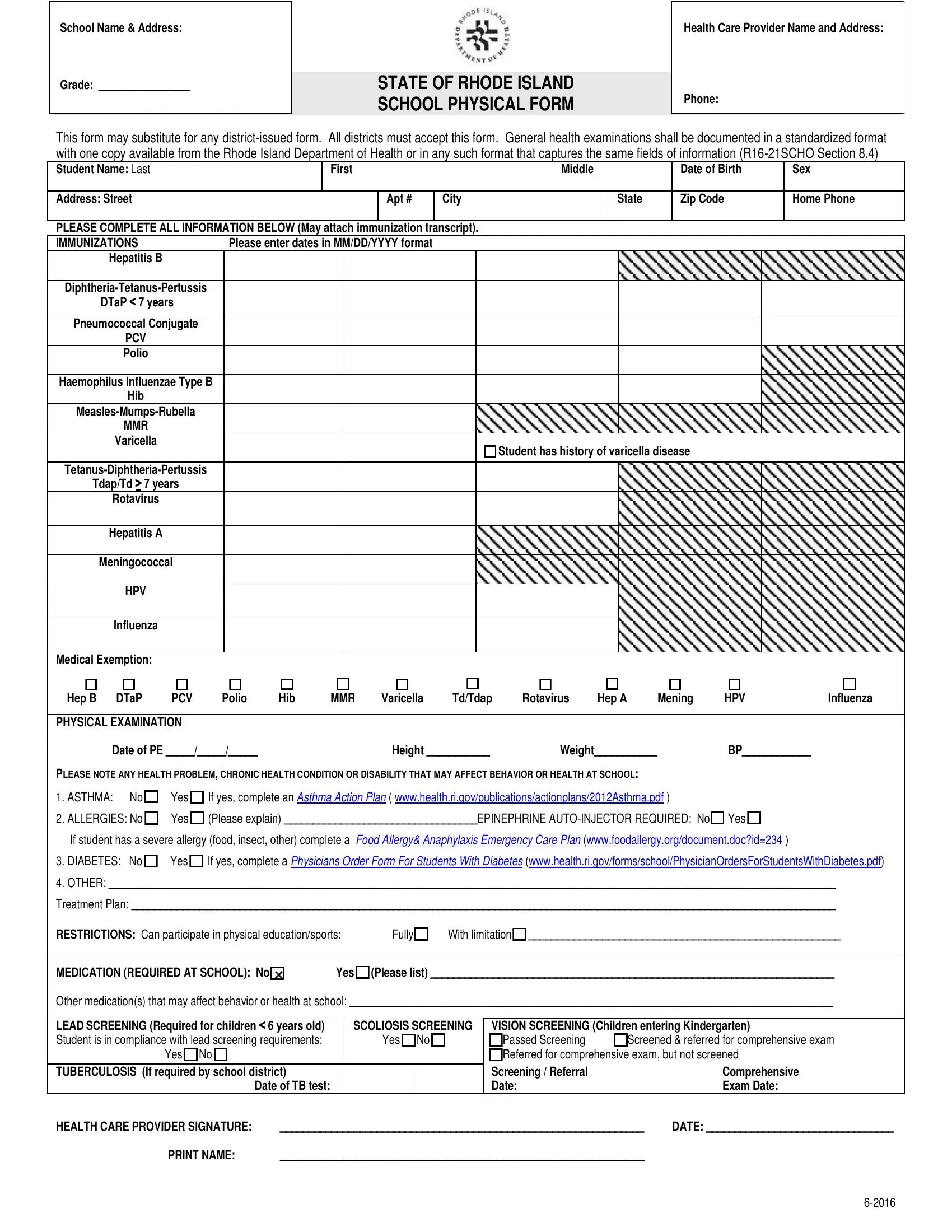
1. While filling out the ri school physical, make certain to incorporate all of the essential fields in its corresponding area. This will help to speed up the process, making it possible for your details to be handled fast and properly.
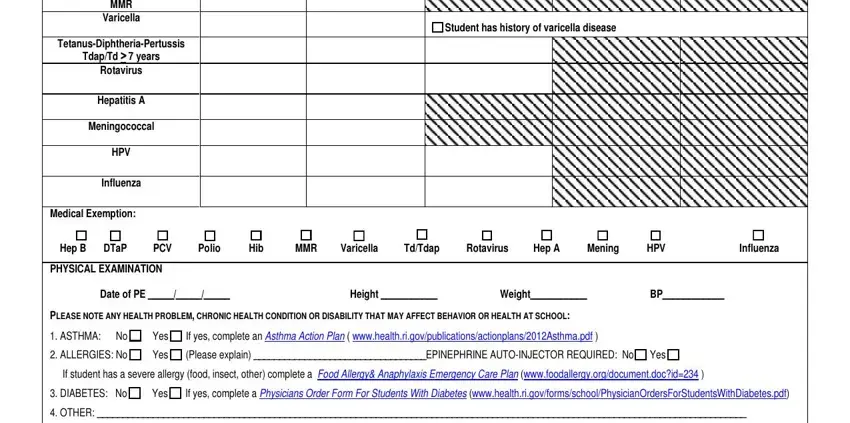
2. After the previous array of fields is done, you have to include the essential particulars in MMR, Varicella, TetanusDiphtheriaPertussis, TdapTd years, Rotavirus, Hepatitis A, Meningococcal, HPV, Influenza, Medical Exemption, Student has history of varicella, Hep B, DTaP, PCV, and Polio so you're able to proceed further.
Be extremely attentive when completing Meningococcal and Hep B, as this is where many people make mistakes.
3. In this particular stage, check out Treatment Plan, RESTRICTIONS Can participate in, Fully, With limitation, MEDICATION REQUIRED AT SCHOOL No, Yes Please list, Other medications that may affect, LEAD SCREENING Required for, SCOLIOSIS SCREENING, Yes No, Yes No, TUBERCULOSIS If required by school, Date of TB test, VISION SCREENING Children entering, and Comprehensive Exam Date. Each of these should be filled out with highest awareness of detail.
Step 3: Prior to finalizing the file, check that blank fields have been filled out the proper way. When you establish that it's good, click “Done." Obtain your ri school physical the instant you subscribe to a 7-day free trial. Readily get access to the pdf file in your personal account, along with any edits and adjustments being all saved! With FormsPal, you'll be able to complete forms without having to get worried about information incidents or data entries being shared. Our secure software helps to ensure that your personal details are stored safe.