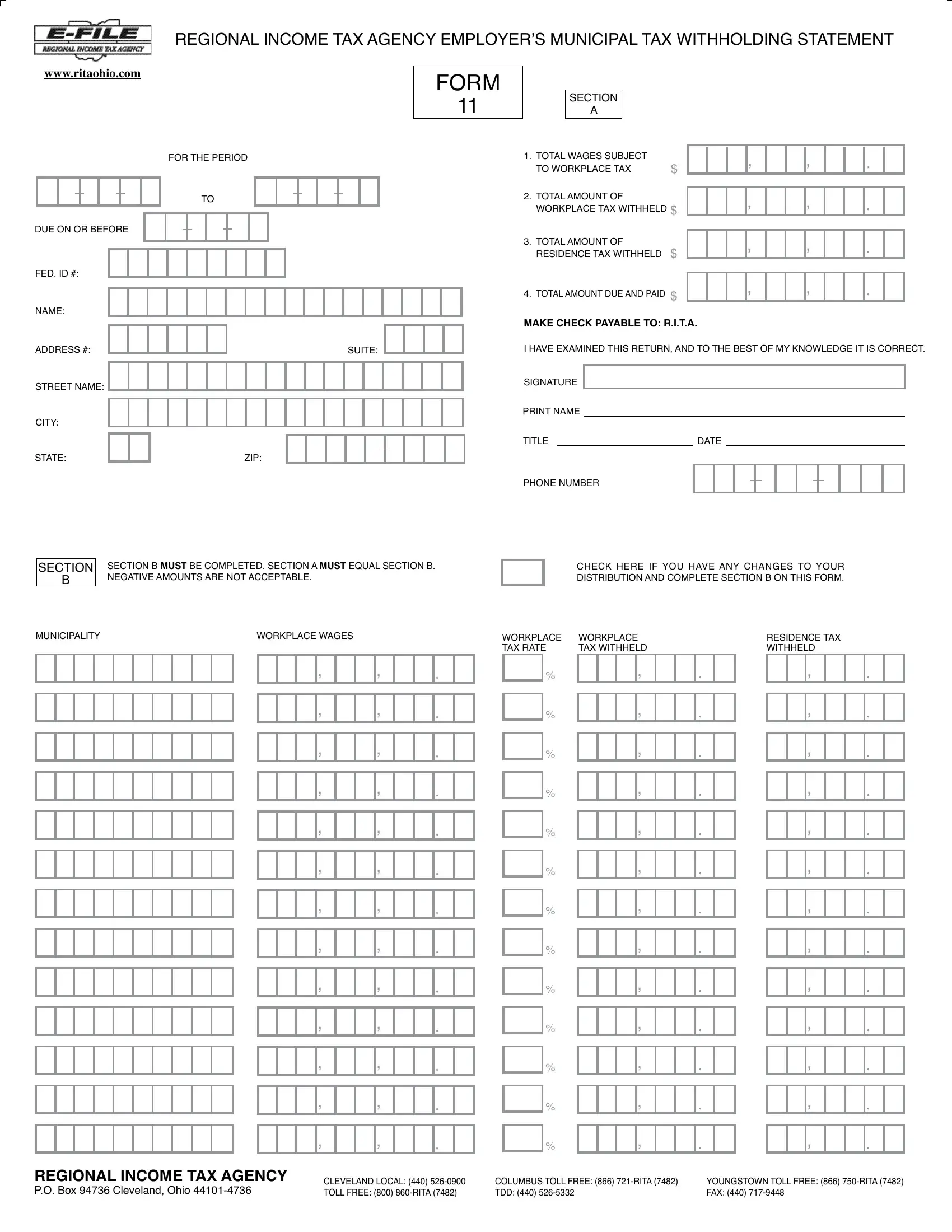
The Regional Income Tax Agency (R.I.T.A.) provides an indispensable tool for employers with its Employer’s Municipal Tax Withholding Statement, widely known as the Rita 11 form. This form serves as a declaration of total wages subject to municipal taxes, the amount withheld for both workplace and residence taxes, and the total due and paid by the employer. Designed to ensure employers accurately remit local taxes withheld from employees' wages, it features a detailed breakdown in Section A for reporting totals and a corresponding Section B for detailed municipality-specific data, emphasizing the necessity of alignment between both sections. Moreover, the form mandates the reconciliation of withheld tax amounts against local tax rates, providing a comprehensive vehicle for compliance with local tax regulations. With sections meticulously designed to capture essential tax withholding information and the form's availability on the R.I.T.A. website, it represents a critical component in the landscape of municipal tax compliance for employers. Additionally, the form facilitates modifications to distribution details if there have been any changes, signifying its adaptability to evolving employer needs. Contact information and payment instructions included in the form underscore the agency's commitment to accessibility and ease of use for employers navigating municipal tax obligations.
| Question | Answer |
|---|---|
| Form Name | Rita Form 11 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | rita form 11 fillable, form 11 rita, form 11 from rita, ritaq forms 11 |
REGIONAL INCOME TAX AGENCY EMPLOYER’S MUNICIPAL TAX WITHHOLDING STATEMENT
WWW.RITAOHIO.COM
FOR THE PERIOD
11LF05A
TO
DUE ON OR BEFORE
FED. ID #:
NAME:
FORM
11
SECTION
A
1. TOTAL WAGES SUBJECT |
|
TO WORKPLACE TAX |
$ |
2.TOTAL AMOUNT OF WORKPLACE TAX WITHHELD $
3.TOTAL AMOUNT OF RESIDENCE TAX WITHHELD $
4.TOTAL AMOUNT DUE AND PAID $
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS #: |
|
|
|
|
|
|
SUITE: |
STREET NAME:
CITY:
STATE: |
|
|
ZIP: |
SECTION SECTION B MUST BE COMPLETED. SECTION A MUST EQUAL SECTION B.
BNEGATIVE AMOUNTS ARE NOT ACCEPTABLE.
MAKE CHECK PAYABLE TO: R.I.T.A.
I HAVE EXAMINED THIS RETURN, AND TO THE BEST OF MY KNOWLEDGE IT IS CORRECT.
SIGNATURE
PRINT NAME
TITLE |
|
DATE |
PHONE NUMBER
CHECK HERE IF YOU HAVE ANY CHANGES TO YOUR
DISTRIBUTION AND COMPLETE SECTION B ON THIS FORM.
MUNICIPALITY |
|
WORKPLACE WAGES |
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
, |
|
|
, |
|
|
. |
|
WORKPLACE TAX RATE
%
%
%
%
%
%
%
%
%
%
%
%
%
WORKPLACE
TAX WITHHELD
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
RESIDENCE TAX
WITHHELD
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
REGIONAL INCOME TAX AGENCY |
CLEVELAND LOCAL: (440) |
|
P.O. BOX 94736 CLEVELAND, OHIO |
||
TOLL FREE: (800) |
COLUMBUS TOLL FREE: (866) |
YOUNGSTOWN TOLL FREE: (866) |
TDD: (440) |
FAX: (440) |
SECTION
B
MUNICIPALITY |
WORKPLACE WAGES |
FORM
11
WORKPLACE |
WORKPLACE |
TAX RATE |
TAX WITHHELD |
11LF05B
RESIDENCE TAX WITHHELD
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
, |
|
|
, |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
%
%
%
%
%
%
%
%
%
%
%
%
%
%
%
%
%
%
%
%
%
%
%
%
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
.
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
,
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
11LF09