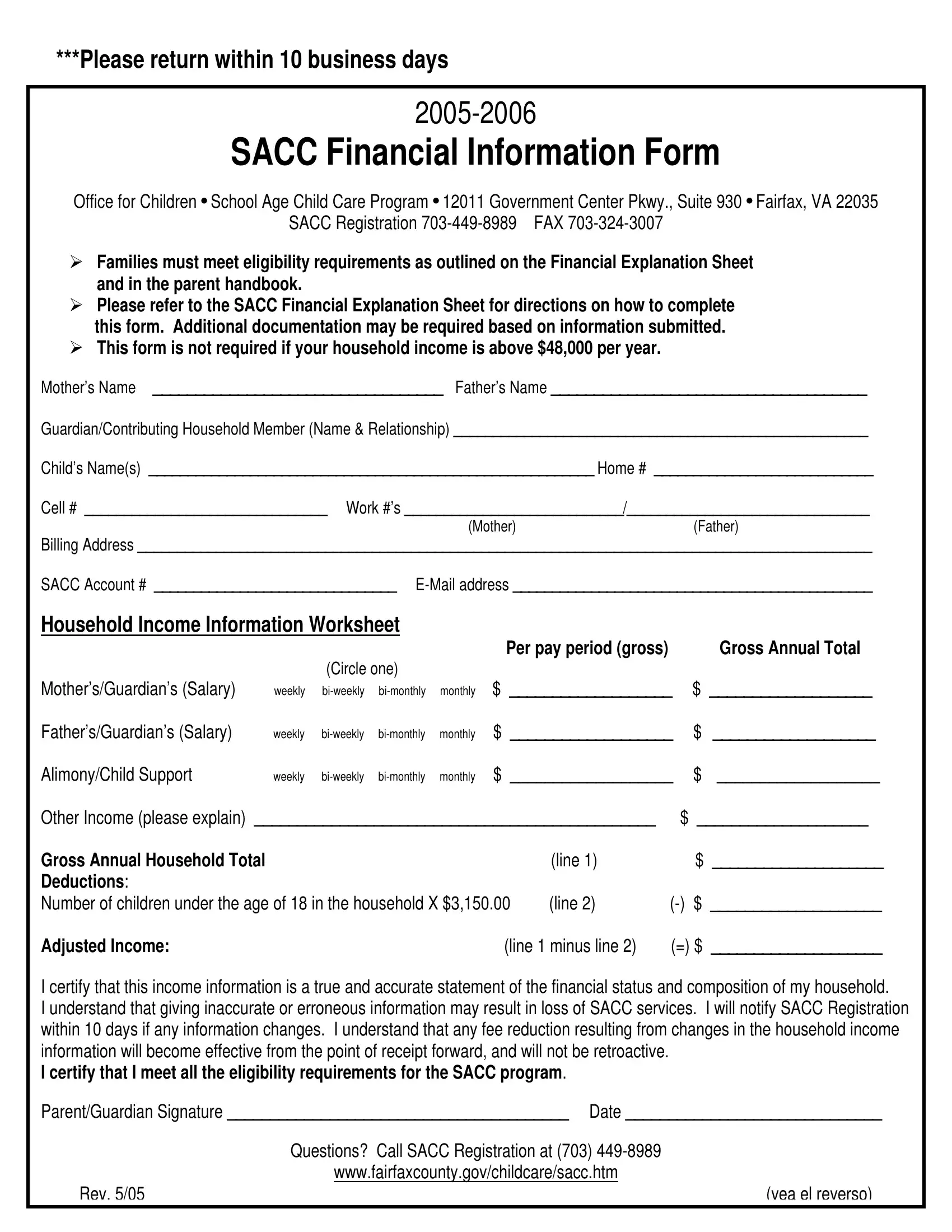
The Sacc Financial Information form serves as a critical tool for families seeking to obtain or maintain eligibility for the School Age Child Care Program (SACC) provided by the Office for Children in Fairfax, VA. This form, which must be returned within ten business days of receipt, requests detailed financial information from the applicant, including household income, to assess eligibility based on outlined criteria. The documentation is designed to cater specifically to those whose household income does not exceed $48,000 per year, demanding precise figures on earnings, the number of children under 18, and any additional sources of income or deductions. It’s a mandatory step for those applying for SACC services, ensuring that the financial assistance provided aligns with the needs of the families it’s meant to support. Additionally, the form includes spaces for both parents' or guardians' names, contributing household members, and the child or children who will be participating in the SACC program. By certifying the accuracy of the information provided, parents or guardians acknowledge the consequences of submitting inaccurate data, which could lead to the loss of SACC services. This form not only aids in the administrative process but emphasizes the importance of transparency and honesty in the application for financial assistance within the SACC program. Applicants are encouraged to connect with SACC Registration for any queries or needed clarification on completing the form. The process underscores Fairfax County’s commitment to providing accessible child care solutions to its residents, ensuring that financial constraints do not hinder children's access to quality care and supervision during crucial out-of-school hours.
| Question | Answer |
|---|---|
| Form Name | Sacc Financial Information Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | fairfaxcounty, sacc form, SACC, sacc application |
***Please return within 10 business days
SACC Financial Information Form
Office for Children • School Age Child Care Program • 12011 Government Center Pkwy., Suite 930 • Fairfax, VA 22035
SACC Registration
Families must meet eligibility requirements as outlined on the Financial Explanation Sheet and in the parent handbook.
Please refer to the SACC Financial Explanation Sheet for directions on how to complete this form. Additional documentation may be required based on information submitted. This form is not required if your household income is above $48,000 per year.
Mother’s Name __________________________________ Father’s Name _____________________________________
Guardian/Contributing Household Member (Name & Relationship) _____________________________________________________
Child’s Name(s) _________________________________________________________ Home # ____________________________
Cell # _______________________________ Work #’s ____________________________/_______________________________
(Mother)(Father)
Billing Address ______________________________________________________________________________________________
SACC Account # _______________________________
Household Income Information Worksheet
Per pay period (gross) |
Gross Annual Total |
(Circle one) |
|
Mother’s/Guardian’s (Salary)
Father’s/Guardian’s (Salary)
Alimony/Child Support
weekly
weekly
weekly
$___________________ $ ___________________
$___________________ $ ___________________
$___________________ $ ___________________
Other Income (please explain) _______________________________________________ |
$ ____________________ |
||
Gross Annual Household Total |
|
(line 1) |
$ ____________________ |
Deductions: |
|
|
|
Number of children under the age of 18 in the household X $3,150.00 |
(line 2) |
||
Adjusted Income: |
(line 1 minus line 2) |
(=) $ ____________________ |
|
I certify that this income information is a true and accurate statement of the financial status and composition of my household.
I understand that giving inaccurate or erroneous information may result in loss of SACC services. I will notify SACC Registration within 10 days if any information changes. I understand that any fee reduction resulting from changes in the household income information will become effective from the point of receipt forward, and will not be retroactive.
I certify that I meet all the eligibility requirements for the SACC program.
Parent/Guardian Signature ________________________________________ Date ______________________________
|
Questions? Call SACC Registration at (703) |
|
www.fairfaxcounty.gov/childcare/sacc.htm |
Rev. 5/05 |
(vea el reverso) |