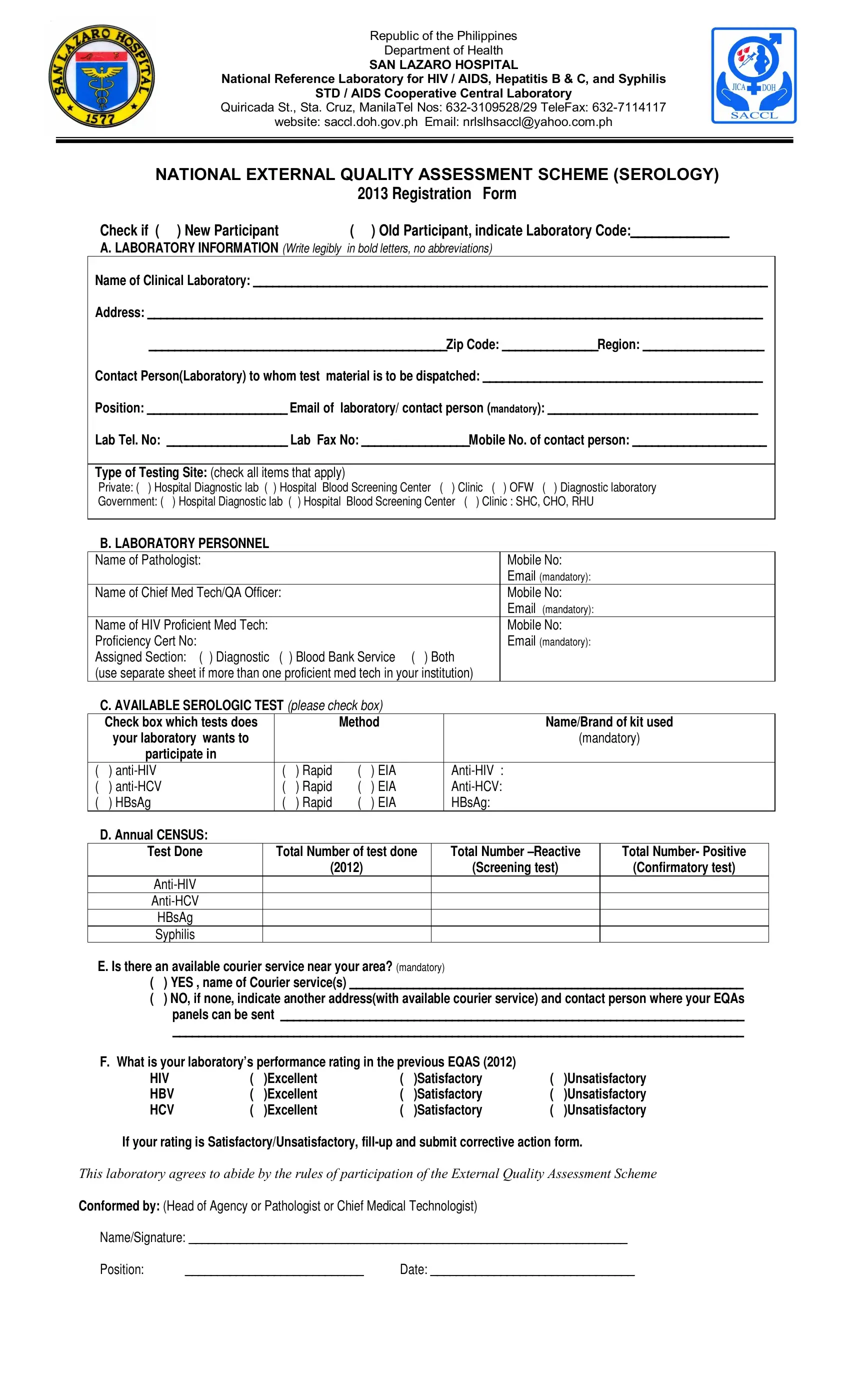
In an effort to elevate the standards of medical testing in the Philippines, particularly for HIV/AIDS, Hepatitis B and C, and Syphilis, the Department of Health has instituted a comprehensive external quality assessment scheme through the San Lazaro Hospital's National Reference Laboratory. Known as the NATIONAL EXTERNAL QUALITY ASSESSMENT SCHEME (SEROLOGY) 2013, this initiative invites participation from clinical laboratories across the nation, whether they are new to the scheme or continuing participants. Laboratories are required to provide detailed information about their operations, including contact details, types of testing sites (be it private or government), and the specific tests they are equipped to perform. Moreover, the form mandates the submission of laboratory personnel credentials and the annual census on the tests conducted, emphasizing the importance of transparency and accountability in medical diagnostics. Laboratories also need to report on the availability of courier services for sending test materials and their performance ratings from previous assessments, highlighting the program's commitment to continuous improvement in laboratory services. This meticulous approach underlines the critical role that accurate and reliable diagnostics play in public health, aiming to ensure the highest quality of care for individuals across the nation.
| Question | Answer |
|---|---|
| Form Name | SACCL DOH Form |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 72 |
| Avg. time to fill out | 14 min 58 sec |
| Other names | ritm, serology neqas 2021, saccl forms, nrl saccl website |
Republic of the Philippines
Department of Health
SAN LAZARO HOSPITAL
National Reference Laboratory for HIV / AIDS, Hepatitis B & C, and Syphilis
STD / AIDS Cooperative Central Laboratory
Quiricada St., Sta. Cruz, ManilaTel Nos:
website: saccl.doh.gov.ph Email: nrlslhsaccl@yahoo.com.ph
NATIONAL EXTERNAL QUALITY ASSESSMENT SCHEME (SEROLOGY)
|
2013 Registration Form |
Check if ( ) New Participant |
( ) Old Participant, indicate Laboratory Code:______________ |
A. LABORATORY INFORMATION (Write legibly in bold letters, no abbreviations)
Name of Clinical Laboratory: _________________________________________________________________________________
Address: _________________________________________________________________________________________________
_______________________________________________Zip Code: _______________Region: ___________________
Contact Person(Laboratory) to whom test material is to be dispatched: ____________________________________________
Position: ______________________ Email of laboratory/ contact person (mandatory): _________________________________
Lab Tel. No: ___________________ Lab Fax No: _________________Mobile No. of contact person: _____________________
Type of Testing Site: (check all items that apply)
Private: ( ) Hospital Diagnostic lab ( ) Hospital Blood Screening Center ( ) Clinic ( ) OFW ( ) Diagnostic laboratory
Government: ( ) Hospital Diagnostic lab ( ) Hospital Blood Screening Center ( ) Clinic : SHC, CHO, RHU
B. LABORATORY PERSONNEL
Name of Pathologist: |
|
|
|
|
|
Mobile No: |
|
|
|
|
|
|
|
|
Email (mandatory): |
Name of Chief Med Tech/QA Officer: |
|
|
|
|
|
Mobile No: |
|
|
|
|
|
|
|
|
Email (mandatory): |
Name of HIV Proficient Med Tech: |
|
|
|
|
|
Mobile No: |
|
Proficiency Cert No: |
|
|
|
|
|
Email (mandatory): |
|
Assigned Section: ( ) Diagnostic ( ) Blood Bank Service ( ) Both |
|
||||||
(use separate sheet if more than one proficient med tech in your institution) |
|
||||||
C. AVAILABLE SEROLOGIC TEST (please check box) |
|
|
|||||
Check box which tests does |
|
|
|
Method |
|
Name/Brand of kit used |
|
your laboratory wants to |
|
|
|
|
|
|
(mandatory) |
participate in |
|
|
|
|
|
|
|
( ) |
|
( |
) Rapid |
( |
) EIA |
||
( ) |
|
( |
) Rapid |
( |
) EIA |
||
( ) HBsAg |
|
( |
) Rapid |
( |
) EIA |
HBsAg: |
|
D. Annual CENSUS:
Test Done |
Total Number of test done |
Total Number |
Total Number- Positive |
|
(2012) |
(Screening test) |
(Confirmatory test) |
|
|
|
|
|
|
|
|
HBsAg |
|
|
|
Syphilis |
|
|
|
E. Is there an available courier service near your area? (mandatory)
( ) YES , name of Courier service(s) ______________________________________________________________
( ) NO, if none, indicate another address(with available courier service) and contact person where your EQAs panels can be sent _________________________________________________________________________
__________________________________________________________________________________________
F. What is your laboratory’s performance rating in the previous EQAS (2012) |
|
|
||||
HIV |
( |
)Excellent |
( |
)Satisfactory |
( |
)Unsatisfactory |
HBV |
( |
)Excellent |
( |
)Satisfactory |
( |
)Unsatisfactory |
HCV |
( |
)Excellent |
( |
)Satisfactory |
( |
)Unsatisfactory |
If your rating is Satisfactory/Unsatisfactory,
This laboratory agrees to abide by the rules of participation of the External Quality Assessment Scheme
Conformed by: (Head of Agency or Pathologist or Chief Medical Technologist)
Name/Signature: _____________________________________________________________________
Position: |
____________________________ |
Date: ________________________________ |
CORRECTIVE ACTION FORM
Name of Laboratory: _____________________________________________________
Lab Code: _____________
Error: __________________________________________________________________
__________________________________________________________________
Action/s Taken to Identify Source of Error:
__________________________________________________________________
__________________________________________________________________
Action/s Taken to Correct Error:
__________________________________________________________________
__________________________________________________________________
Comments:
__________________________________________________________________
__________________________________________________________________
_________________________________ Date____________
Name/Signature of Medical Technologist
_________________________________ Date____________
Name/Signature of Supervisor/Pathologist