
Using PDF forms online can be a breeze with our PDF editor. Anyone can fill out scdot claim here and use many other functions we offer. The tool is continually improved by us, receiving additional features and growing to be greater. Here is what you will have to do to begin:
Step 1: Press the "Get Form" button at the top of this webpage to access our tool.
Step 2: The tool offers you the opportunity to work with your PDF file in various ways. Modify it with personalized text, correct original content, and add a signature - all possible in no time!
This document will require specific info to be entered, hence be sure to take some time to provide what's requested:
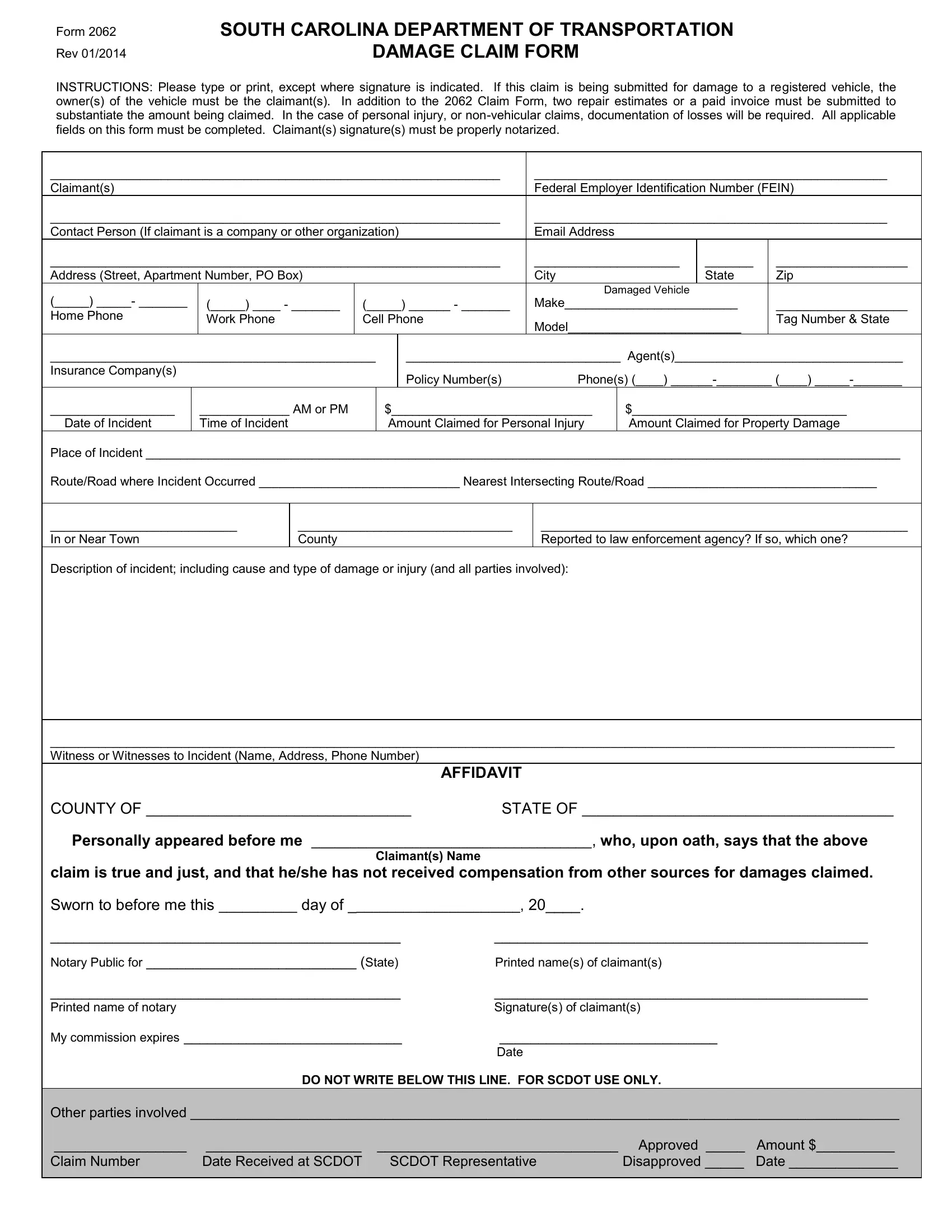
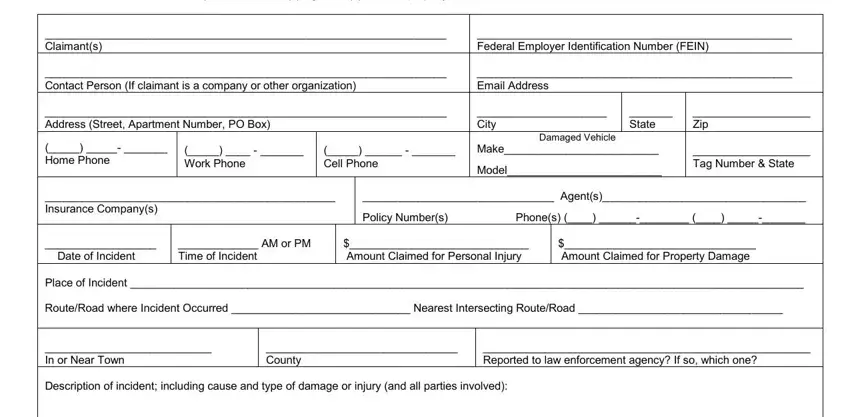
1. To begin with, when completing the scdot claim, begin with the section that features the subsequent fields:
2. The third step would be to complete these blanks: Date of Incident Place of, AFFIDAVIT, COUNTY OF STATE OF Personally, Notary Public for State Printed, DO NOT WRITE BELOW THIS LINE FOR, and Other parties involved.
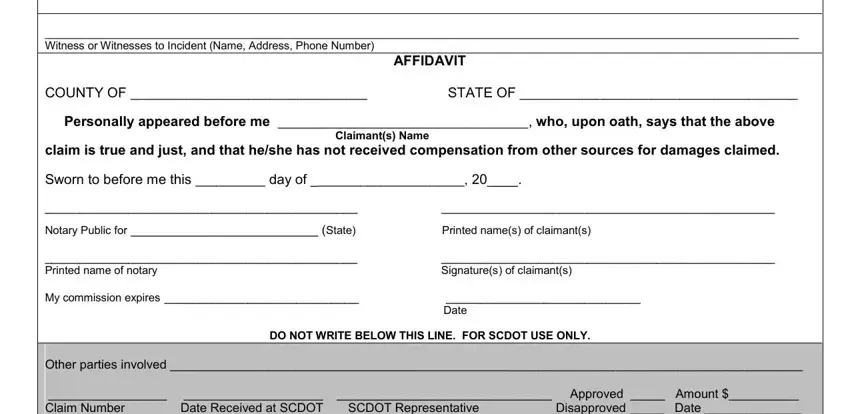
In terms of Date of Incident Place of and Other parties involved, make sure you take a second look in this current part. These two are definitely the most important ones in the PDF.
Step 3: Spell-check the details you have inserted in the form fields and then hit the "Done" button. After setting up afree trial account with us, it will be possible to download scdot claim or email it directly. The PDF will also be accessible through your personal cabinet with your every modification. FormsPal is devoted to the personal privacy of all our users; we make sure all information put into our system is secure.