
With the online editor for PDFs by FormsPal, it is possible to fill out or alter Legal Malpractice Claim Report Form here. To make our editor better and simpler to utilize, we consistently implement new features, taking into account suggestions coming from our users. To start your journey, take these basic steps:
Step 1: Hit the "Get Form" button at the top of this page to open our tool.
Step 2: With our state-of-the-art PDF editor, it's possible to do more than merely fill in forms. Try all of the features and make your docs appear sublime with custom text put in, or tweak the file's original input to perfection - all that supported by the capability to insert stunning pictures and sign the file off.
This PDF form will need specific details; to ensure accuracy, don't hesitate to pay attention to the following guidelines:
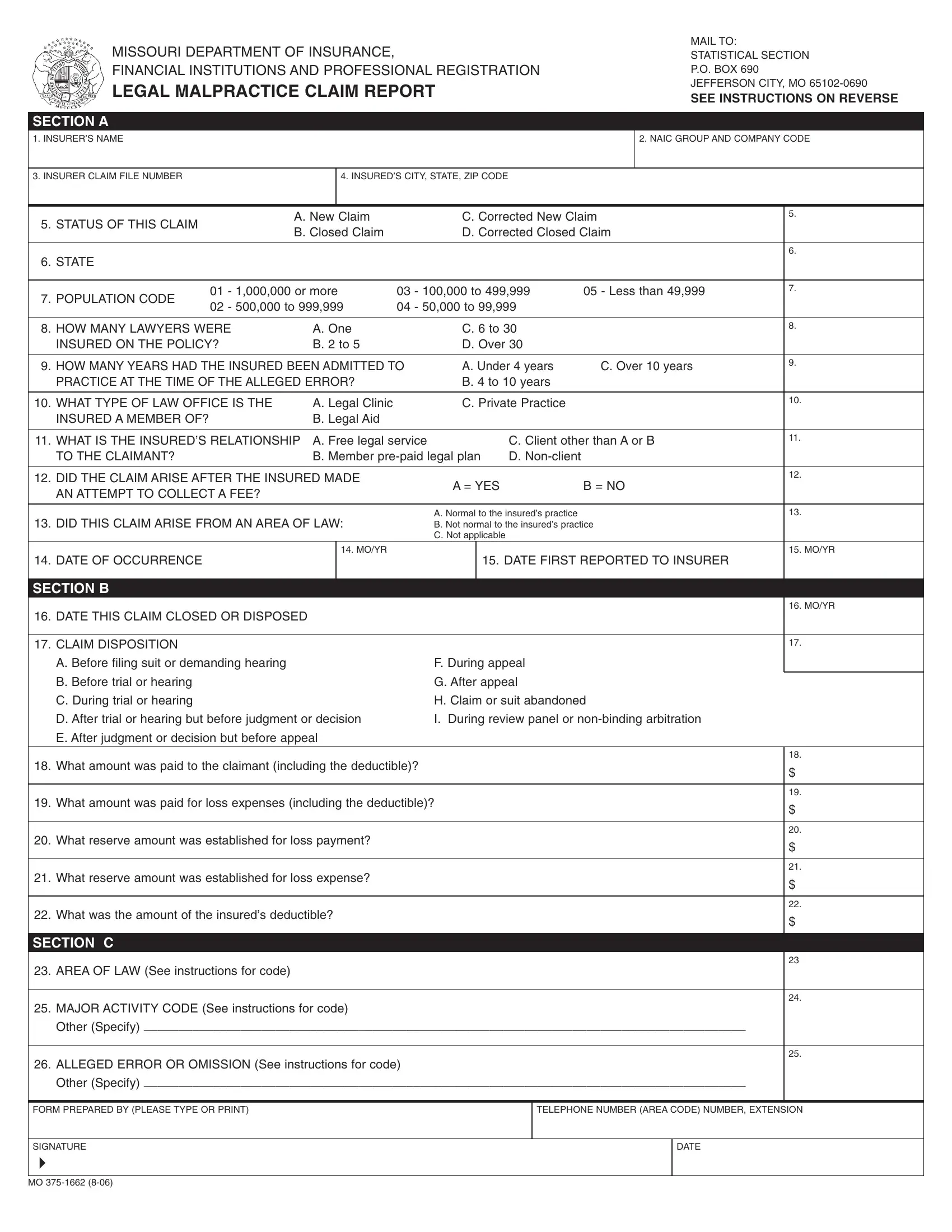
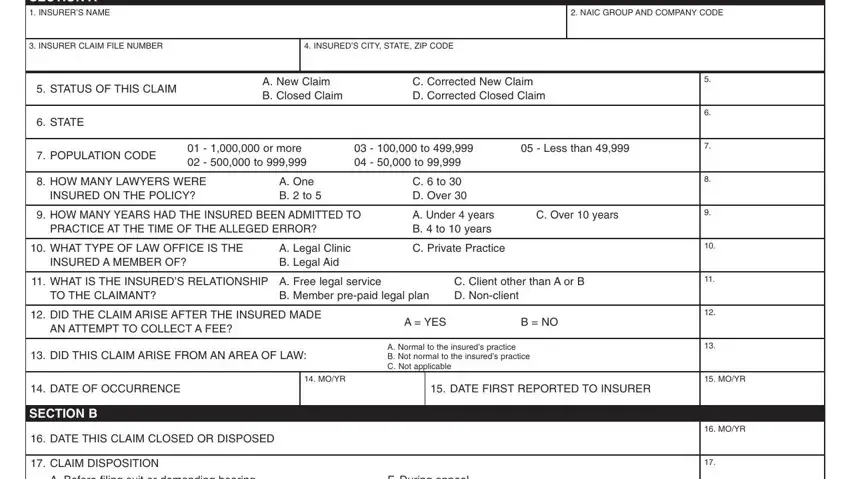
1. To start with, while filling out the Legal Malpractice Claim Report Form, start out with the section that has the subsequent fields:
2. Once your current task is complete, take the next step – fill out all of these fields - E After judgment or decision but, What amount was paid to the, What amount was paid for loss, What reserve amount was, What reserve amount was, What was the amount of the, SECTION C, AREA OF LAW See instructions for, MAJOR ACTIVITY CODE See, Other Specify, ALLEGED ERROR OR OMISSION See, Other Specify, FORM PREPARED BY PLEASE TYPE OR, TELEPHONE NUMBER AREA CODE NUMBER, and SIGNATURE with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
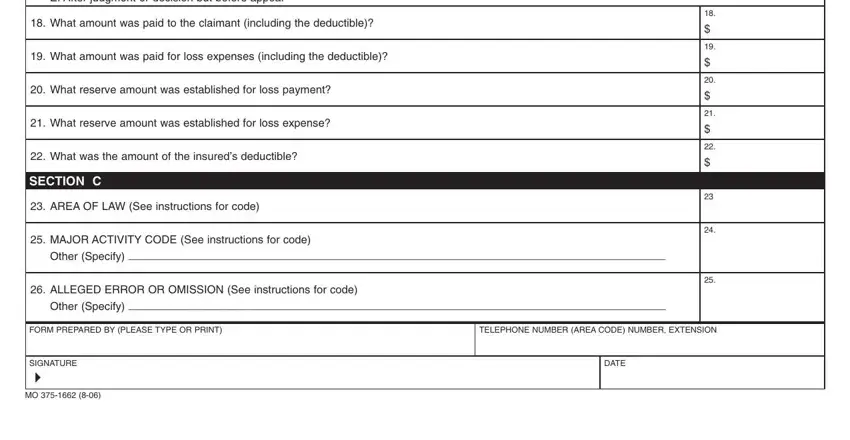
It's easy to get it wrong while filling out the ALLEGED ERROR OR OMISSION See, consequently be sure to go through it again before you decide to submit it.
Step 3: After going through the filled in blanks, hit "Done" and you're good to go! After starting a7-day free trial account here, it will be possible to download Legal Malpractice Claim Report Form or email it promptly. The PDF document will also be easily accessible through your personal account with all your edits. FormsPal is committed to the privacy of all our users; we make certain that all personal information entered into our editor is kept protected.