
With the online editor for PDFs by FormsPal, you can easily fill in or modify medcore ipa referral form here and now. To maintain our editor on the cutting edge of convenience, we strive to adopt user-driven capabilities and improvements regularly. We are at all times grateful for any suggestions - play a pivotal role in revolutionizing PDF editing. It merely requires a couple of easy steps:
Step 1: Just click on the "Get Form Button" above on this page to start up our pdf form editor. Here you'll find all that is needed to work with your file.
Step 2: With this handy PDF editing tool, you can actually do more than just fill in blanks. Express yourself and make your docs appear professional with custom textual content incorporated, or fine-tune the file's original input to excellence - all supported by an ability to add almost any photos and sign it off.
This PDF doc needs some specific details; in order to ensure accuracy and reliability, make sure you consider the following suggestions:
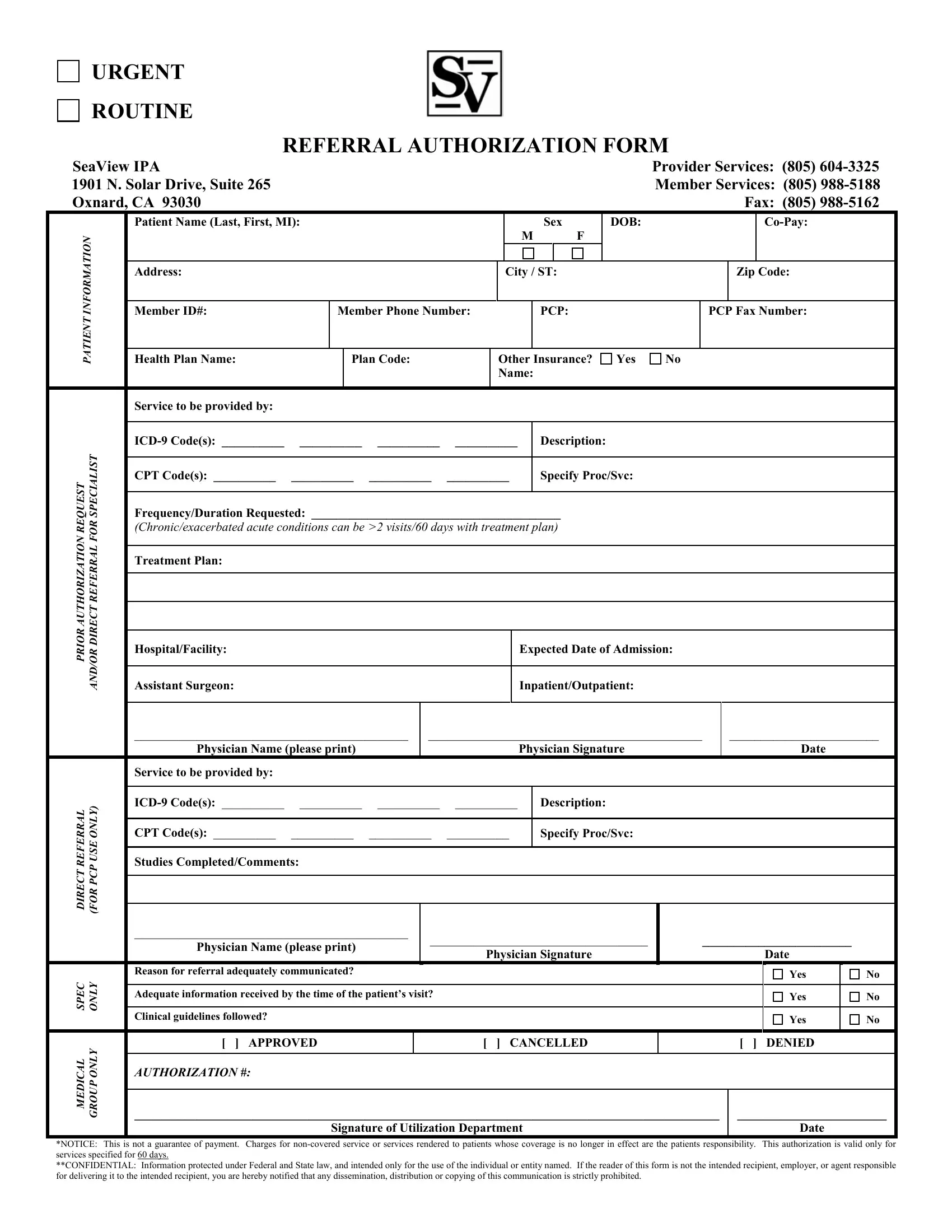
1. For starters, while filling out the medcore ipa referral form, start with the form section with the following blanks:
2. Soon after this part is done, go to enter the relevant information in all these - T S I L A I C E P S R O F L A R R, FrequencyDuration Requested, Treatment Plan, HospitalFacility, Assistant Surgeon, Expected Date of Admission, InpatientOutpatient, Physician Name please print, Physician Signature, Date, T S E U Q E R N O I T A Z I R O H, L A R R E F E R T C E R I D, Y L N O E S U P C P R O F, Service to be provided by, and ICD Codes.
Be really attentive while filling out Expected Date of Admission and Physician Signature, because this is the part where many people make some mistakes.
3. The next step is typically quite easy, Reason for referral adequately, C E P S, Y L N O, Adequate information received by, Clinical guidelines followed, Yes, Yes, Yes, L A C I D E M, Y L N O P U O R G, APPROVED, CANCELLED, DENIED, AUTHORIZATION, and Signature of Utilization Department - all of these form fields needs to be completed here.
Step 3: Ensure the details are accurate and press "Done" to complete the process. After registering afree trial account with us, it will be possible to download medcore ipa referral form or send it via email immediately. The PDF will also be easily accessible in your personal cabinet with your each and every edit. We don't share any details you provide whenever working with forms at FormsPal.