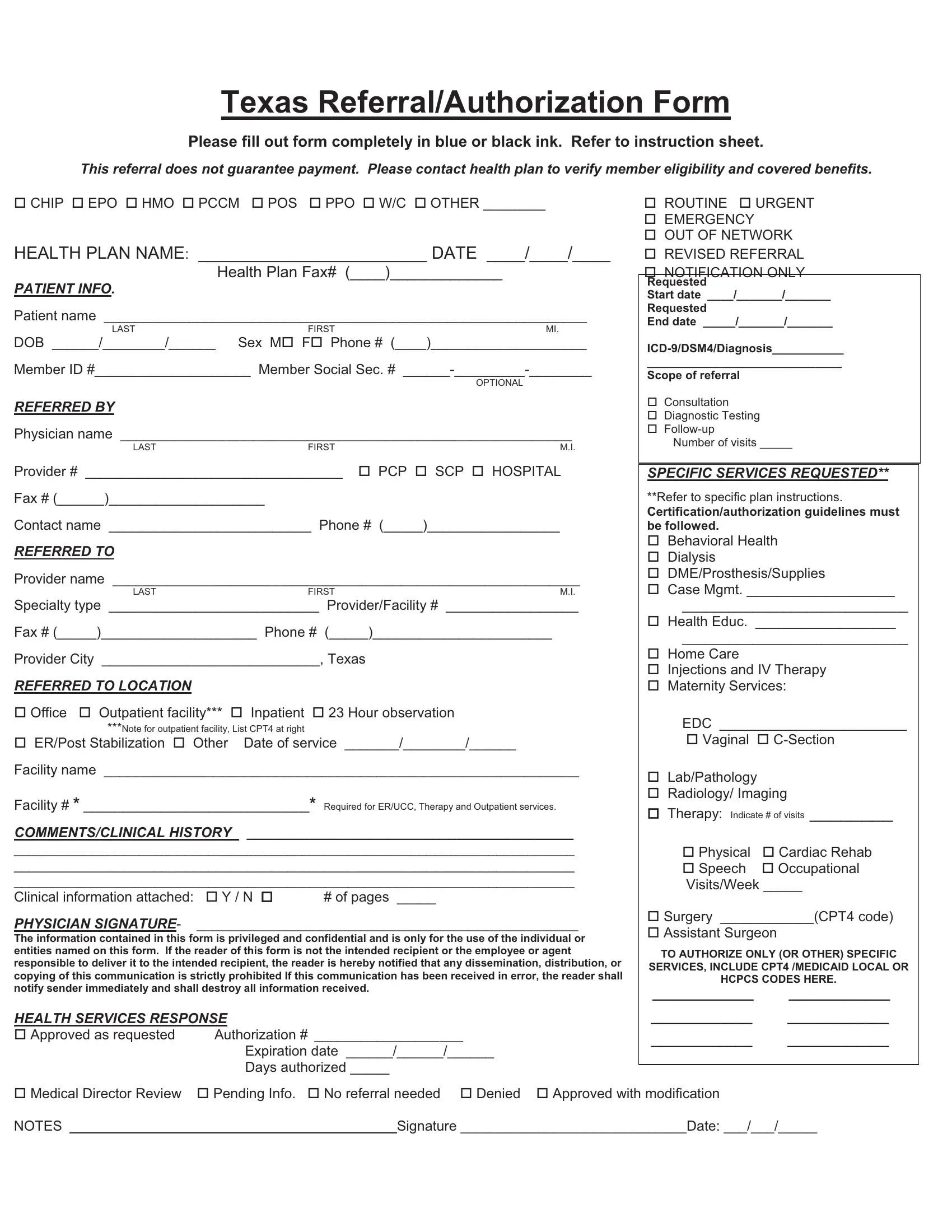
In navigating the complexities of healthcare coverage, the Texas Referral/Authorization Form emerges as a crucial document for both patients and healthcare providers. This comprehensive form, to be filled out with precise attention using blue or black ink, guides the submission process for varying types of healthcare plans, including but not limited to CHIP, EPO, HMO, PCCM, POS, PPO, and others. It mandates the submission of detailed patient information, referral sources, and targeted provider details, aiming to streamline the communication between healthcare entities and insurance plans. By instructing users to verify member eligibility and benefit coverage with their respective health plans, it underscores the reality that a referral does not inherently guarantee payment. Alongside capturing essential data — like patient demographics, referring and referred to provider information, and service specifications — this form also makes room for comments on clinical history and the attaching of pertinent clinical documents. Its segments on health services response highlight the sense of urgency and the scope of the referral, ranging from routine to emergency, and clarifies the process for approval or denial. This all-encompassing approach not only aids in the effective referral of patients within Texas but also emphasizes the importance of detailed communications and adherence to specific plan instructions for successful healthcare service authorization.
| Question | Answer |
|---|---|
| Form Name | Referral Authorization Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | outside referral form parkland hospital, parklabd referral form, parkland referrals, parkland outside referral form |
