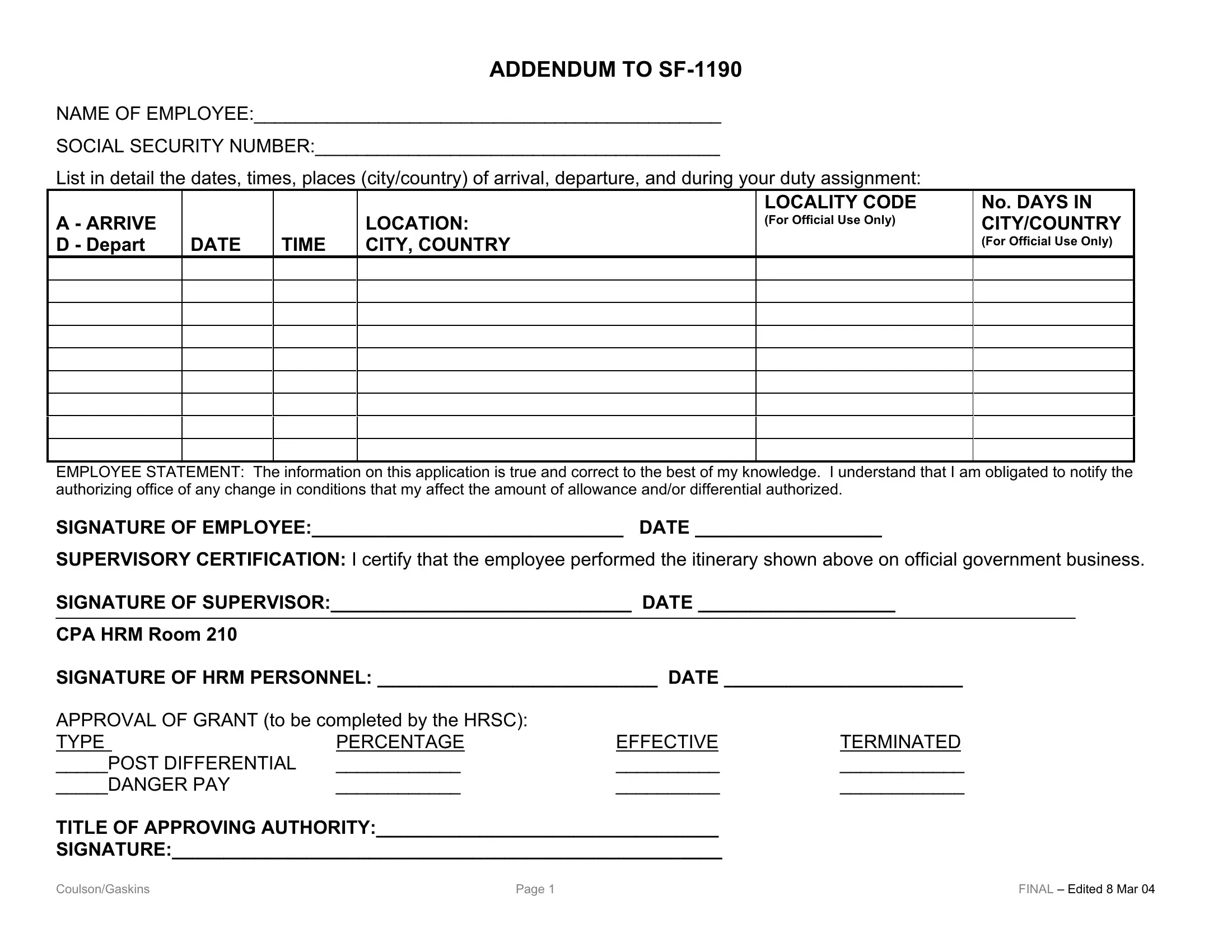
Understanding the intricacies of government paperwork is crucial for employees involved in international assignments, and one such document that frequently arises in this context is the SF-1190 form, an Addendum for Foreign Allowances Application, Grant and Report. Primarily, it serves as a detailed record for employees to report specifics about their travel and duty assignments abroad, including the dates, times, and locations (city/country) involved in their itineraries. This form also plays a vital role in determining eligibility and calculating certain allowances or differentials, such as post differential and danger pay, aimed at compensating employees for the unique challenges posed by international assignments. By requiring the employee's statement to affirm the truthfulness of the provided information and endorsements from supervisory and Human Resources Management (HRM) personnel, the SF-1190 ensures accountability and accuracy in the allowance application process. It is essential for employees and their supervisors to familiarize themselves with this form and its requirements, as it directly impacts the financial and administrative aspects of overseas assignments. Recognizing the significance of correct and prompt submission can greatly affect the smooth conduct of governmental operations across borders.
| Question | Answer |
|---|---|
| Form Name | Sf 1190 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | sf 1190 fillable, sf 1190 addendum fillable form, addendum 1190, sf form 1190 addendum |
ADDENDUM TO
NAME OF EMPLOYEE:_____________________________________________
SOCIAL SECURITY NUMBER:_______________________________________
List in detail the dates, times, places (city/country) of arrival, departure, and during your duty assignment:
A - ARRIVE D - Depart
DATE
TIME
LOCATION: CITY, COUNTRY
LOCALITY CODE
(For Official Use Only)
No. DAYS IN CITY/COUNTRY
(For Official Use Only)
EMPLOYEE STATEMENT: The information on this application is true and correct to the best of my knowledge. I understand that I am obligated to notify the authorizing office of any change in conditions that my affect the amount of allowance and/or differential authorized.
SIGNATURE OF EMPLOYEE:______________________________ DATE __________________
SUPERVISORY CERTIFICATION: I certify that the employee performed the itinerary shown above on official government business.
SIGNATURE OF SUPERVISOR:_____________________________ DATE ___________________
CPA HRM Room 210
SIGNATURE OF HRM PERSONNEL: ___________________________ DATE _______________________
APPROVAL OF GRANT (to be completed by the HRSC): |
|
|
|
TYPE |
PERCENTAGE |
EFFECTIVE |
TERMINATED |
_____POST DIFFERENTIAL |
____________ |
__________ |
____________ |
_____DANGER PAY |
____________ |
__________ |
____________ |
TITLE OF APPROVING AUTHORITY:_________________________________
SIGNATURE:_____________________________________________________
Coulson/Gaskins |
Page 1 |
FINAL – Edited 8 Mar 04 |