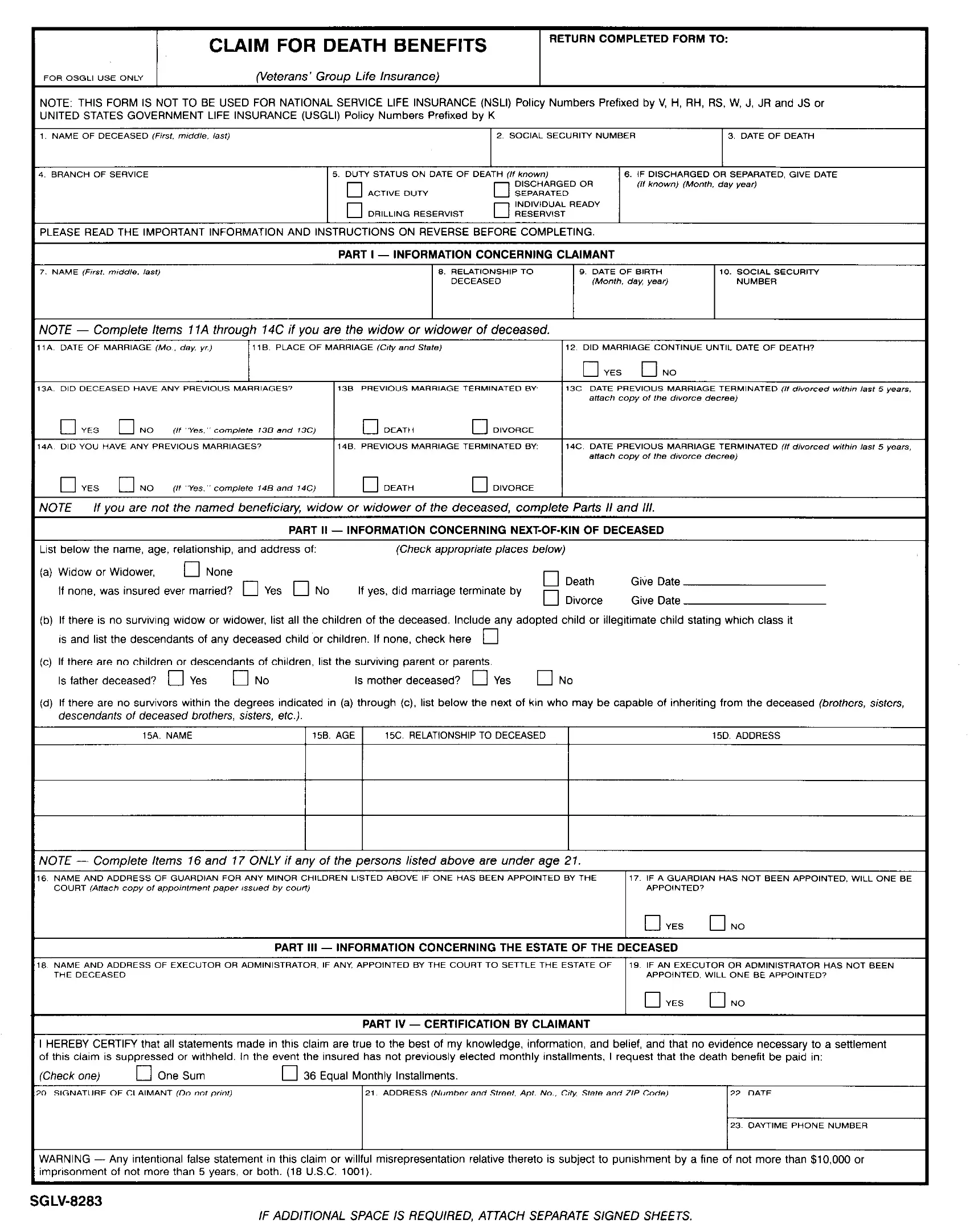
The SGLV 8283 form, known as the Claim for Death Benefits, plays a pivotal role for families navigating the challenging times following the loss of a loved one who served in the United States armed forces. Designed for beneficiaries under the Servicemen’s Group Life Insurance (SGLI) and Veterans’ Group Life Insurance (VGLI) policies, it sets the process in motion to secure vital financial support posthumously. The form clarifies it is not applicable for National Service Life Insurance or United States Government Life Insurance policies, marking a clear boundary on its applicability. Detailed instructions ensure claimants provide all necessary information, including the full name and Social Security number of the deceased, date and details of death, plus the claimant's relationship and identifying information. It emphasizes the importance of furnishing complete and accurate details to prevent delays in claim processing, with a caution against the submission of false information under penalty of law. For those who are primary beneficiaries, like spouses or children, as well as for those who might inherit in the absence of a named beneficiary, the document outlines a clear hierarchy of recipients, ensuring that the benefits reach the hands of those intended. With required evidence varying based on the deceased's service status at the time of death, the form also guides users on the necessary documentation to accompany claims, simplifying a process that can seem daunting during a period of grief.
| Question | Answer |
|---|---|
| Form Name | Sglv 8283 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 8283 form sglv, form 8283 sglv, sglv8283 form print, sglv 8283 forms |
