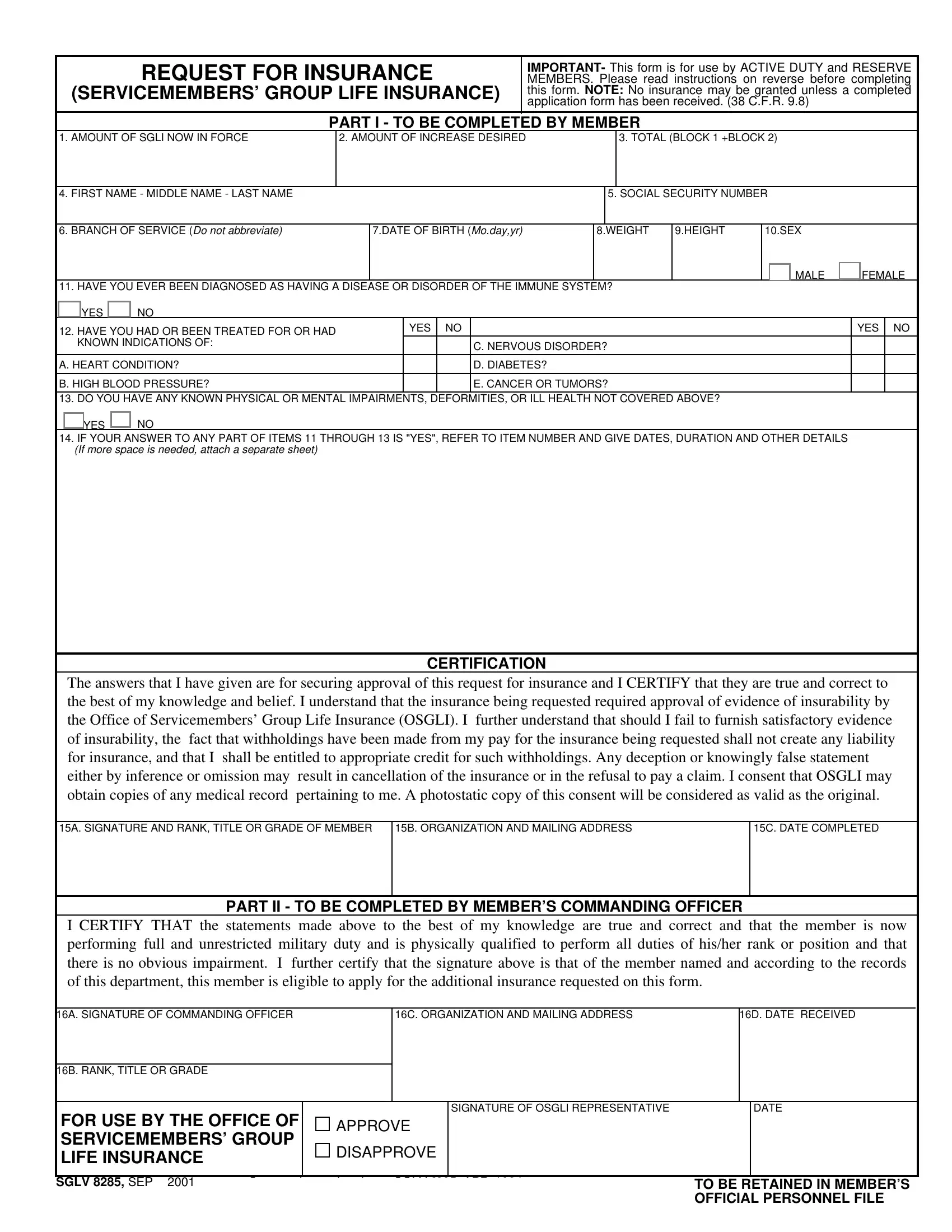
REQUEST FOR INSURANCE
(SERVICEMEMBERS’ GROUP LIFE INSURANCE)
IMPORTANT- This form is for use by ACTIVE DUTY and RESERVE MEMBERS. Please read instructions on reverse before completing this form. NOTE: No insurance may be granted unless a completed application form has been received. (38 C.F.R. 9.8)
PART I - TO BE COMPLETED BY MEMBER
1. AMOUNT OF SGLI NOW IN FORCE
2. AMOUNT OF INCREASE DESIRED
3. TOTAL (BLOCK 1 +BLOCK 2)
4. FIRST NAME - MIDDLE NAME - LAST NAME
5. SOCIAL SECURITY NUMBER
|
|
|
|
|
|
|
|
|
|
|
|
6. BRANCH OF SERVICE (Do not abbreviate) |
7.DATE OF BIRTH (Mo.day,yr) |
|
8.WEIGHT |
9.HEIGHT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11. HAVE YOU EVER BEEN DIAGNOSED AS HAVING A DISEASE OR DISORDER OF THE IMMUNE SYSTEM?
|
YES |
|
NO |
YES |
|
NO |
|
12. HAVE YOU HAD OR BEEN TREATED FOR OR HAD |
|
|
|
|
|
|
KNOWN INDICATIONS OF: |
|
|
|
C. NERVOUS DISORDER? |
|
|
|
|
|
|
|
A. HEART CONDITION? |
|
|
|
D. DIABETES? |
B. HIGH BLOOD PRESSURE? |
|
|
|
E. CANCER OR TUMORS? |
|
|
|
|
|
|
|
|
13. DO YOU HAVE ANY KNOWN PHYSICAL OR MENTAL IMPAIRMENTS, DEFORMITIES, OR ILL HEALTH NOT COVERED ABOVE?
YES NO
14.IF YOUR ANSWER TO ANY PART OF ITEMS 11 THROUGH 13 IS "YES", REFER TO ITEM NUMBER AND GIVE DATES, DURATION AND OTHER DETAILS (If more space is needed, attach a separate sheet)
CERTIFICATION
The answers that I have given are for securing approval of this request for insurance and I CERTIFY that they are true and correct to the best of my knowledge and belief. I understand that the insurance being requested required approval of evidence of insurability by the Office of Servicemembers’ Group Life Insurance (OSGLI). I further understand that should I fail to furnish satisfactory evidence of insurability, the fact that withholdings have been made from my pay for the insurance being requested shall not create any liability for insurance, and that I shall be entitled to appropriate credit for such withholdings. Any deception or knowingly false statement either by inference or omission may result in cancellation of the insurance or in the refusal to pay a claim. I consent that OSGLI may obtain copies of any medical record pertaining to me. A photostatic copy of this consent will be considered as valid as the original.
15A. SIGNATURE AND RANK, TITLE OR GRADE OF MEMBER
15B. ORGANIZATION AND MAILING ADDRESS
PART II - TO BE COMPLETED BY MEMBER’S COMMANDING OFFICER
I CERTIFY THAT the statements made above to the best of my knowledge are true and correct and that the member is now performing full and unrestricted military duty and is physically qualified to perform all duties of his/her rank or position and that there is no obvious impairment. I further certify that the signature above is that of the member named and according to the records of this department, this member is eligible to apply for the additional insurance requested on this form.
16A. SIGNATURE OF COMMANDING OFFICER
16C. ORGANIZATION AND MAILING ADDRESS
16B. RANK, TITLE OR GRADE |
|
|
|
|
|
|
|
|
|
|
|
|
|
FOR USE BY THE OFFICE OF |
|
SIGNATURE OF OSGLI REPRESENTATIVE |
|
DATE |
APPROVE |
|
|
|
|
SERVICEMEMBERS’ GROUP |
|
|
|
|
DISAPPROVE |
|
|
|
|
LIFE INSURANCE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SGLV 8285, SEP 2001 |
Supersedes and replaces SGLV 8285, APR 1994, |
|
TO BE RETAINED IN MEMBER’S |
|
Which will not be used. |
|
OFFICIAL PERSONNEL FILE |
|
|
|
|
|
IMPORTANT
Use this form to apply for:
1.Restoration of Servicemembers’ Group Life Insurance if you previously cancelled or declined coverage, or
2.For increasing the amount of Servicemembers’ Group Life Insurance coverage if you have less than the maximum amount.
If you already have some Servicemembers’ Group Life Insurance, any beneficiary you named for that insurance will become the beneficiary of the additional insurance also. If you want a different beneficiary or if you do not already have some Servicemembers’ Group Life Insurance, obtain VA Form SGLV 8286, Servicemembers’ Group Life Insurance Election and Certificate, and file it with your organization.
INSTRUCTIONS - PLEASE READ CAREFULLY BEFORE COMPLETING THIS FORM
TO MEMBER - Complete and sign this form. Answer all questions by typing or printing in ink. Remember, your total insurance may not exceed $400,000. If you do not know, or are not sure of your current SGLI in force, put the total amount of coverage you desire in BLOCK 3. Then submit the form for completion by your Commanding Officer. If this request is accepted, the insurance will be effective as of the date you submit it for completion. Premiums will automatically be deducted from your pay.
TO UNIFORMED SERVICE - This form should be completed and signed by the member. It should then be certifed below the member’s signature by his/her Commanding Officer or equivalent superior.
If the member’s answers are "NO" to Item 11, all parts of Item 12 and to Item 13, the completed form should be retained in the member’s personnel file. Once this is done, action should be initiated to deduct premiums from the member’s pay. It is not necessary to send a copy of this form to the Office of Servicemembers’ Group Life Insurance (OSGLI) for approval. However, a copy of the completed form is to be forwarded to OSGLI in the event of the member’s death.
If the member answers "YES" to Item 11, or to any part of Item 12, or to Item 13, the original is to be filed in the member’s personnel file and a copy of the completed form sent to the:
Office of Servicemembers’ Group life Insurance
PO BOX 41618
PHILA., PA 19176-9913
Upon receipt, OSGLI will review the application and return an annotated copy to the member’s organization showing whether the request is approved or disapproved. The copy returned from OSGLI is to be filed in the member’s personnel file. No action should be taken to deduct the premium from the member’s pay until the "APPROVED" form is received from OSGLI. At this time, the premium deduction should be made effective as of the date that the SGLV 8285 was submitted. (Note: If the member dies between the time the form is submitted to OSGLI and the time it is returned marked "APPROVED", the insurance will be paid. If the form is returned marked "DISAPPROVED", the insurance will not be paid.) If the request for insurance is disapproved, the member should be notified and advised that he/she may write to OSGLI or telephone them at 1-800-419-1473 for an explanation.