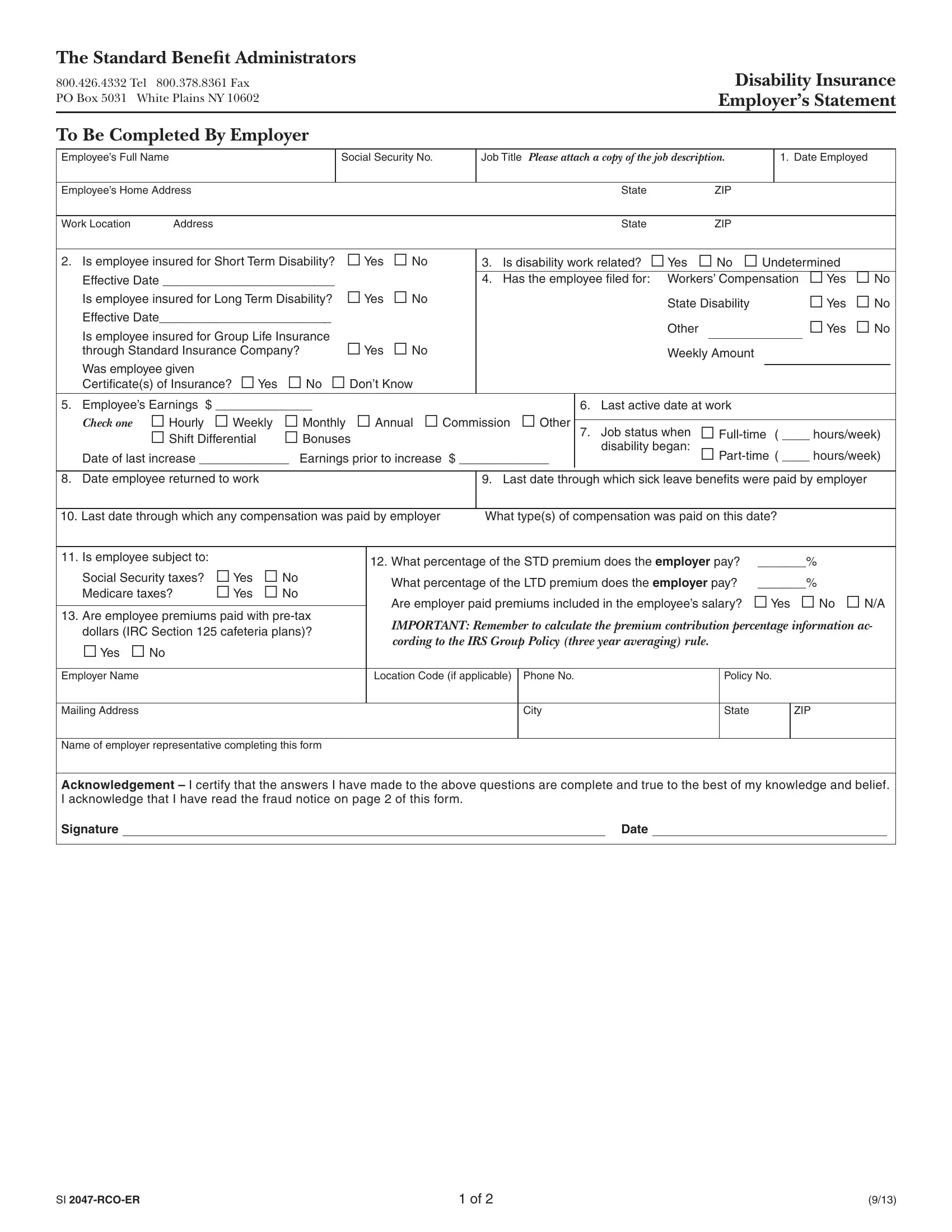
Navigating the intricacies of disability insurance claims can often seem daunting for both employers and employees alike. The Si 2047 Rco Er form plays a crucial role in this process, serving as an essential document for Standard Benefit Administrators. Specifically designed for employers to complete, this form collects comprehensive information about an employee's claim for disability benefits, including personal details, employment history, insurance coverage status, and the nature of the disability. Employers are required to disclose whether the employee is covered under short-term, long-term, or group life insurance policies, and whether these insurances were provided through Standard Insurance Company. Additionally, the form inquires about the work-relatedness of the disability, any workers’ compensation filed, the employee’s earnings, job status at the onset of disability, and the return-to-work status. It also touches on the employer's contribution towards the disability premiums, the taxation status of these premiums, and whether the premiums are paid with pre-tax dollars. Moreover, the form incorporates fraud notices for residents of various states, highlighting the legal penalties for submitting false or misleading information. This form not only facilitates the processing of disability claims but also underscores the legal obligations and potential consequences for all parties involved.
| Question | Answer |
|---|---|
| Form Name | Si 2047 Rco Er Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | CALIFORNIA, insurer, RHODE, hereto |
The Standard Benefit Administrators
800.426.4332 Tel 800.378.8361 Fax |
Disability Insurance |
PO Box 5031 White Plains NY 10602 |
Employer’s Statement |
To Be Completed By Employer |
|
Employee’s Full Name
Social Security No.
Job Title Please attach a copy of the job description.
1. Date Employed
Employee’s Home Address |
State |
ZIP |
|
|
|
|
|
Work Location |
Address |
State |
ZIP |
2. Is employee insured for Short Term Disability? |
Yes |
No |
Effective Date _________________________ |
|
|
Is employee insured for Long Term Disability? |
Yes |
No |
Effective Date_________________________ |
|
|
Is employee insured for Group Life Insurance |
Yes |
No |
through Standard Insurance Company? |
Was employee given
Certificate(s) of Insurance? Yes No Don’t Know
3. |
Is disability work related? Yes No Undetermined |
|
|
|||
4. |
Has the employee filed for: Workers’ Compensation |
Yes |
No |
|||
|
State Disability |
Yes |
No |
|||
|
Other |
Yes |
No |
|||
|
|
|
|
|
|
|
|
Weekly Amount |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. Employee’s Earnings $ ______________
Check one Hourly Weekly Monthly Annual Commission Other Shift Differential Bonuses
Date of last increase _____________ Earnings prior to increase $ _____________
6.Last active date at work
7.Job status when
8. Date employee returned to work
9. Last date through which sick leave benefits were paid by employer
10. Last date through which any compensation was paid by employer |
What type(s) of compensation was paid on this date? |
||||||
|
|
|
|
|
|
|
|
11. Is employee subject to: |
|
|
12. What percentage of the STD premium does the employer pay? |
_______% |
|||
|
|
|
|||||
Social Security taxes? |
Yes |
No |
What percentage of the LTD premium does the employer pay? |
_______% |
|||
Medicare taxes? |
Yes |
No |
|||||
Are employer paid premiums included in the employee’s salary? |
Yes No N/A |
||||||
|
|
|
|||||
13. Are employee premiums paid with |
|||||||
IMPORTANT: Remember to calculate the premium contribution percentage information ac- |
|||||||
dollars (IRC Section 125 cafeteria plans)? |
|||||||
cording to the IRS Group Policy (three year averaging) rule. |
|
|
|||||
Yes No |
|
|
|
|
|||
|
|
|
|
|
|
||
|
|
|
|
|
|||
Employer Name |
|
|
Location Code (if applicable) Phone No. |
Policy No. |
|||
|
|
|
|
|
|
|
|
Mailing Address
City
State
ZIP
Name of employer representative completing this form
Acknowledgement – I certify that the answers I have made to the above questions are complete and true to the best of my knowledge and belief. I acknowledge that I have read the fraud notice on page 2 of this form.
Signature |
|
Date |
SI |
1 of 2 |
(9/13) |
The Standard Benefit Administrators
800.426.4332 Tel 800.378.8361 Fax |
Disability Insurance |
PO Box 5031 White Plains NY 10602 |
Claim Form Fraud Notices |
Some states require us to provide the following information to you:
ALABAMA, MARYLAND AND RHODE ISLAND RESIDENTS
Any person who knowingly or willfully presents a false or fraudulent claim for payment of a loss or benefit or who knowingly or willfully presents false information in an application for insurance is guilty of a crime and may be subject to fines and confinement in prison.
CALIFORNIA RESIDENTS
For your protection, California law requires the following to appear on this form: Any person who knowingly presents a false or fraudulent claim for the payment of a loss is guilty of a crime and may be subject to fines and confinement in state prison.
COLORADO RESIDENTS
It is unlawful to knowingly provide false, incomplete or misleading facts or information to an insurance company for the purpose of defrauding or attempting to defraud the company. Penalties may include imprisonment, fines, denial of insurance, and civil damages. Any insurance company or agent of an insurance company who knowingly provides false, incomplete, or misleading facts or information to the policyholder or claimant for the purpose of defrauding or attempting to defraud the policyholder or claimant with regard to a settlement or award payable from insurance proceeds shall be reported to the Colorado division of insurance within the department of regulatory agencies.
DISTRICT OF COLUMBIA RESIDENTS
WARNING: It is a crime to provide false or misleading information to an insurer for the purpose of defrauding the insurer or any other person. Penalties include imprisonment and/or fines. In addition, an insurer may deny insurance benefits, if false information materially related to a claim was provided by the applicant.
FLORIDA RESIDENTS
Any person who knowingly and with intent to injure, defraud or deceive an insurance company, files a statement of claim or an application containing false, incomplete or misleading information is guilty of a felony of the third degree
NEW JERSEY RESIDENTS
Any person who knowingly files a statement of claim containing any false or misleading information is subject to criminal and civil penalties.
NEW YORK RESIDENTS
Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance or statement of claim, containing any materially false information, or conceals for the purpose of misleading, information concerning any fact material thereto, commits a fraudulent insurance act, which is a crime, and shall also be subject to civil penalty not to exceed five thousand dollars and the stated value of the claim for each such violation.
PENNSYLVANIA RESIDENTS
Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance or statement of claim containing any materially false information or conceals for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime and subjects such person to criminal and civil penalties.
ALL OTHER RESIDENTS
Some states require us to inform you that any person who knowingly and with intent to injure, defraud or deceive an insurance company, or other person, files a statement containing false or misleading information concerning any fact material hereto commits a fraudulent insurance act which is subject to civil and/or criminal penalties, depending upon the state. Such actions may be deemed a felony and substantial fines may be imposed.
SI |
2 of 2 |
(9/13) |