
It won't be a challenge to fill out application food form working with our PDF editor. This is how you can easily successfully build your file.
Step 1: Step one is to click the orange "Get Form Now" button.
Step 2: Now you may edit the application food form. Feel free to use our multifunctional toolbar to insert, eliminate, and alter the content of the form.
Prepare the application food form PDF and enter the content for every single area:
Include the essential data in the mail, US, Department, of, Agriculture fax, or and email, program, in, take, usda, gov segment.
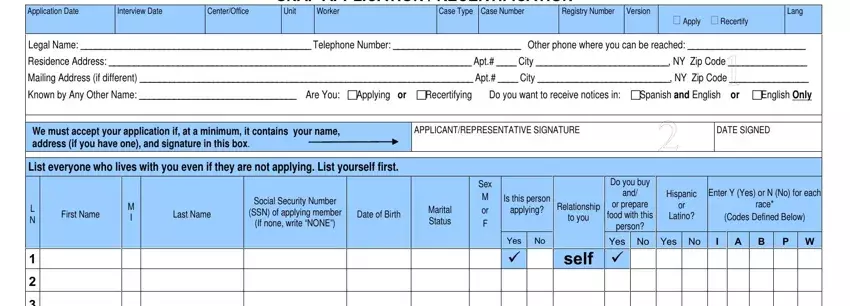
In the Application, Date Interview, Date Center, Office SNAP, APPLICATION, RECERTIFICATION, Unit Case, Number Case, Type Worker, Registry, Number Version, Apply, Re, certify Lang, APPLICANT, REPRESENTATIVE, SIGNATURE DATE, SIGNED Is, this, person and applying, Relationship section, focus on the significant data.
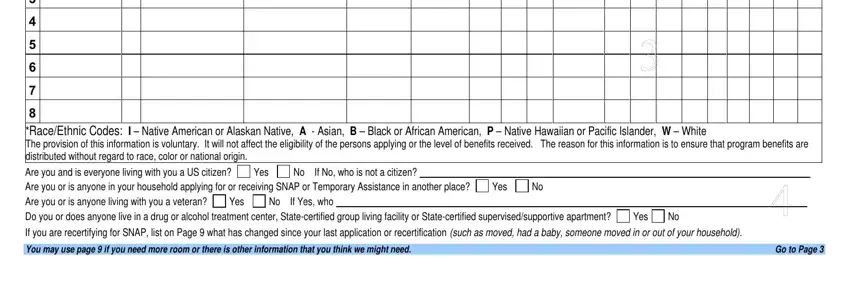
Inside the paragraph Yes, No No, If, No, who, is, not, a, citizen No, If, Yes, who Yes, Yes, Yes, Yes, and Goto, Page include the rights and responsibilities of the sides.
Look at the sections for, example, weekly, biweekly monthly, Before, Deductions Yes, No, If, Yes, explain, on, Page No, If, Yes, who F, Name Yes, Yes, Yes, Yes, No, If, Yes, who and RESOURCES and next fill them out.
Step 3: Select the Done button to save the file. At this point it is ready for transfer to your gadget.
Step 4: It can be safer to have copies of your form. There is no doubt that we are not going to share or read your data.
