Form SSA-521 (07-2023) UF |
|
|
Discontinue Prior Editions |
|
Page 1 of 2 |
Social Security Administration |
TOE 420 |
OMB No. 0960-0015 |
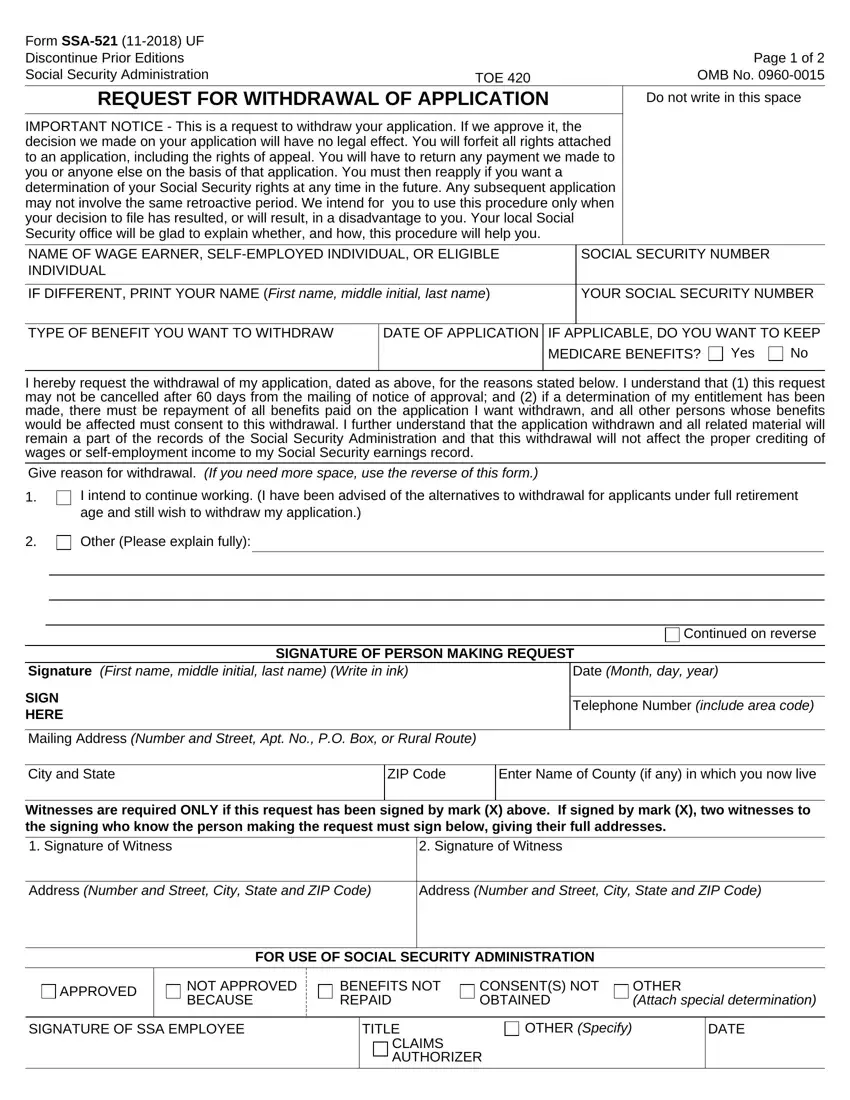
REQUEST FOR WITHDRAWAL OF APPLICATION |
Do not write in this space |
IMPORTANT NOTICE - This is a request to withdraw your application. If we approve it, the decision we made on your application will have no legal effect. You will forfeit all rights attached to an application, including the rights of appeal. You will have to return any payment we made to you or anyone else on the basis of that application. You must then reapply if you want a determination of your Social Security rights at any time in the future. Any subsequent application may not involve the same retroactive period. We intend for you to use this procedure only when your decision to file has resulted, or will result, in a disadvantage to you. Your local Social Security office will be glad to explain whether, and how, this procedure will help you.
|
|
|
|
|
|
|
|
NAME OF WAGE EARNER, SELF-EMPLOYED INDIVIDUAL, OR ELIGIBLE INDIVIDUAL |
|
|
SOCIAL SECURITY NUMBER |
|
|
|
|
|
|
IF DIFFERENT, PRINT YOUR NAME (First name, middle initial, last name) |
YOUR SOCIAL SECURITY NUMBER |
|
|
|
|
TYPE OF BENEFIT YOU WANT TO WITHDRAW |
DATE OF APPLICATION IF |
APPLICABLE, DO YOU WANT TO KEEP |
|
|
MEDICARE BENEFITS? Yes |
No |
I hereby request the withdrawal of my application, dated as above, for the reasons stated below. I understand that (1) this request may not be canceled after 60 days from the mailing of notice of approval; and (2) if a determination of my entitlement has been made, there must be repayment of all benefits paid on the application I want withdrawn, and all other persons whose benefits would be affected must consent to this withdrawal. I further understand that the application withdrawn and all related material will remain a part of the records of the Social Security Administration and that this withdrawal will not affect the proper crediting of wages or self-employment income to my Social Security earnings record.
Give reason for withdrawal. (If you need more space, see additional remarks)
1.I intend to continue working. (I have been advised of the alternatives to withdrawal for applicants under full retirement age and still wish to withdraw my application.)
2. |
Other (Please explain fully): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
See additional remarks
I declare under penalty of perjury that I have examined all the information on this form, and on any accompanying statements or forms, and it is true and correct to the best of my knowledge. I understand that anyone who knowingly gives a false statement about a material fact in this information, or causes someone else to do so, commits a crime and may be subject to a fine or imprisonment.
|
|
|
|
|
|
|
|
|
SIGNATURE OF PERSON MAKING REQUEST |
Signature (First name, middle initial, last name) (Write in ink) |
|
Date (Month, day, year) |
|
SIGN |
|
|
|
|
|
|
|
|
Telephone Number (include area code) |
|
HERE |
|
|
|
|
|
|
|
|
|
|
|
|
Mailing Address (Number and Street, Apt. No., P.O. Box, or Rural Route) |
|
|
|
|
|
|
|
|
|
|
City and State |
|
ZIP Code |
Enter Name of County (if any) in which you now live |
|
|
|
|
|
|
|
|
Witnesses are required ONLY if this request has been signed by mark (X) above. If signed by mark (X), two witnesses to the signing who know the person making the request must sign below, giving their full addresses.
Address (Number and Street, City, State and ZIP Code)
Address (Number and Street, City, State and ZIP Code)
FOR USE OF SOCIAL SECURITY ADMINISTRATION
 APPROVED Signature Field
APPROVED Signature Field
BENEFITS NOT |
CONSENT(S) NOT |
OTHER |
REPAID |
OBTAINED |
(Attach special determination) |
|
TITLE |
OTHER (Specify) |
|
DATE |
|
CLAIMS SPECIALIST |
|
|
|
|
|
|
|
Form SSA-521 (07-2023) UF |
Page 2 of 2 |
|
|
|
|
Additional Remarks: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Privacy Act Statement
Collection and Use of Personal Information
Sections 202, 205, 223 and 1872 of the Social Security Act, as amended, allow us to collect this information. Furnishing us this information is voluntary. However, failing to provide all or part of the information may prevent withdrawal of the application for benefits.
We will use the information you provide to cancel your application for benefits. We may also share the information for the following purposes, called routine uses:
•To contractors and other Federal Agencies, as necessary, for the purpose of assisting us in the efficient administration of our programs. We will disclose information under this routine use only in situations in which we may enter into a contractual or similar agreement to obtain assistance in accomplishing an SSA function relating to this system of records; and,
•To student volunteers, individuals working under a personal services contract, and other workers who technically do not have the status of Federal employees, when they are performing work for us, as authorized by law, and they need access to personally identifiable information (PII) in our records in order to perform their assigned agency functions.
In addition, we may share this information in accordance with the Privacy Act and other Federal laws. For example, where authorized, we may use and disclose this information in computer matching programs, in which our records are compared with other records to establish or verify a person's eligibility for Federal benefit programs and for repayment of incorrect or delinquent debts under these programs.
A list of additional routine uses is available in our Privacy Act System of Records Notice (SORN) 60-0089, entitled, Claims Folders System, as published in the Federal Register (FR) on October 31, 2019, at 84 FR 58422. Additional information, and a full listing of all of our SORNs, is available on our website at www.ssa.gov/privacy.
Paperwork Reduction Act Statement - This information collection meets the requirements of 44 U.S.C. § 3507, as amended by section 2 of the Paperwork Reduction Act of 1995. You do not need to answer these questions unless we display a valid Office of Management and Budget control number. We estimate that it will take about 5 minutes to read the instructions, gather the facts, and answer the questions. SEND OR BRING THE COMPLETED FORM TO YOUR LOCAL SOCIAL SECURITY OFFICE. You can find your local Social Security office through SSA's website at www.socialsecurity.gov. Offices are also listed under U. S. Government agencies in your telephone directory or you may call Social Security at 1-800-772-1213 (TTY 1-800-325-0778).
You may send comments regarding this burden estimate or any other aspect of this collection, including suggestions for reducing this burden to: SSA, 6401 Security Blvd, Baltimore, MD 21235-6401. Send only comments relating to our time estimate or other aspects of this collection to this address, not the completed form.