
You could work with michigan form sos 258 easily in our online PDF editor. FormsPal is aimed at providing you the best possible experience with our editor by regularly presenting new functions and improvements. With these improvements, working with our editor gets better than ever before! With just several easy steps, you can start your PDF editing:
Step 1: Access the form inside our tool by pressing the "Get Form Button" at the top of this page.
Step 2: When you launch the file editor, there'll be the form prepared to be filled in. Aside from filling out various fields, you may as well perform various other actions with the Document, that is adding any words, changing the initial textual content, inserting illustrations or photos, putting your signature on the PDF, and more.
In order to finalize this document, ensure you type in the necessary details in each and every field:
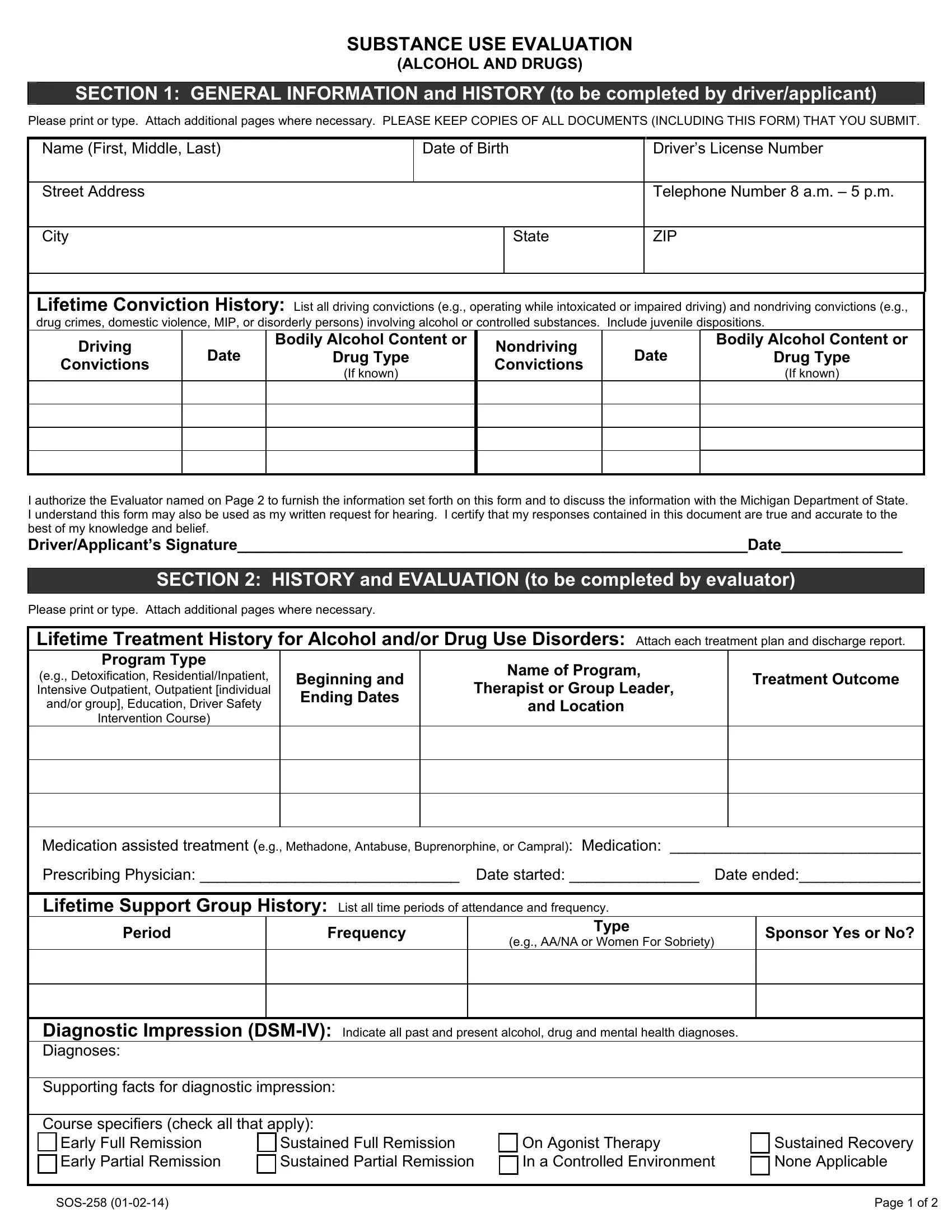
1. While submitting the michigan form sos 258, be sure to incorporate all needed blank fields within its relevant section. It will help to speed up the work, allowing for your information to be handled without delay and appropriately.
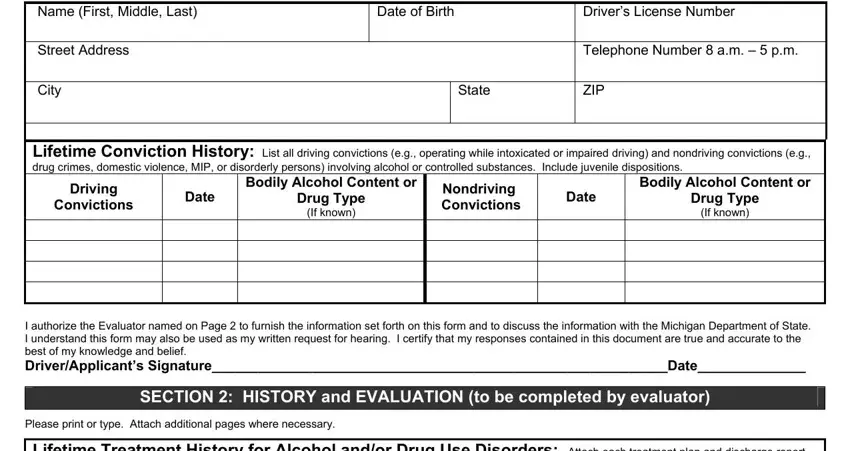
2. The subsequent step would be to submit all of the following fields: andor group Education Driver Safety, Intervention Course, and Location, Beginning and Ending Dates, Medication assisted treatment eg, Period, Frequency, Type, eg AANA or Women For Sobriety, Diagnostic Impression DSMIV, Sustained Full Remission Sustained, On Agonist Therapy In a Controlled, SOS, Sponsor Yes or No, and Sustained Recovery None Applicable.
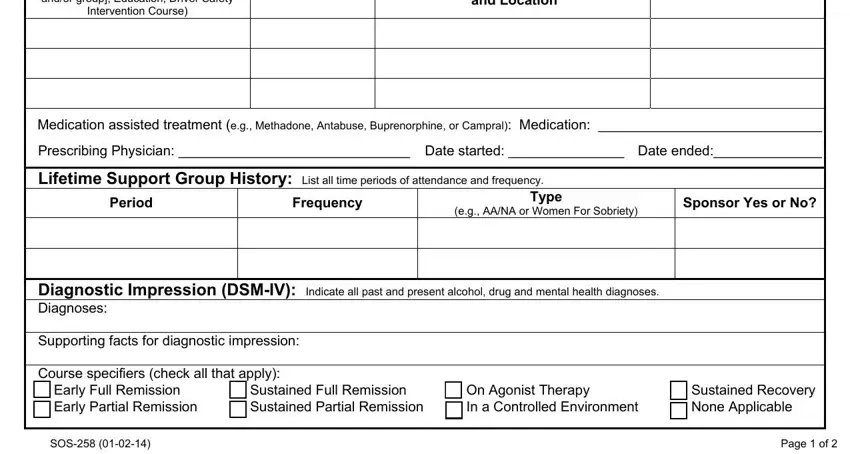
3. The following step is related to Testing Instruments Attach the, Interpretation of results, Explain how the results of this, correlate with the DSMIV diagnosis, Drug Screen Administer a panel, Abstinence Period Abated by What, alcohol controlled substance or NA, Period of Abstinence Beginning and, and Comments - fill out every one of these fields.
Concerning Abstinence Period Abated by What and Comments, make sure you do everything correctly in this current part. These could be the key fields in the PDF.
4. The next paragraph arrives with these particular form blanks to consider: Client Prognosis Please check one, Alcohol andor NA Beer, Controlled SubstancesInclude, Date of last use of Continuum of, Educational Course, Reasons for recommendation or if, Community Support Group eg AANA, Other, None, Certification of Evaluator As of, QualificationsDegrees, Telephone Number, and Date.
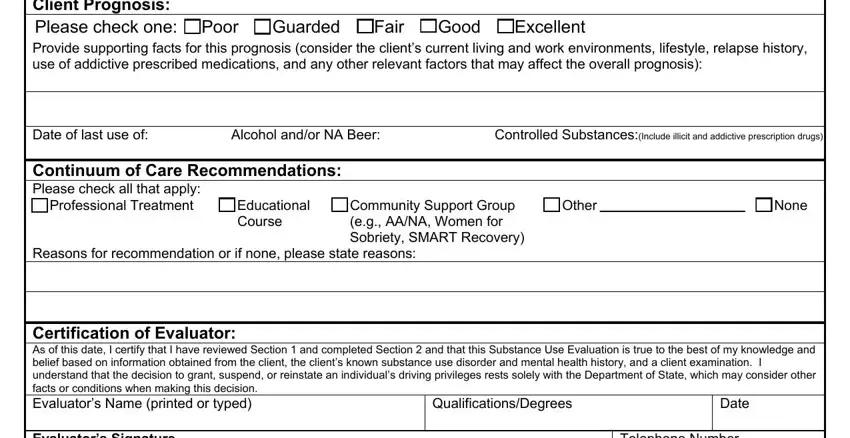
5. This last step to finalize this document is essential. You must fill in the displayed blanks, and this includes Certification of Evaluator As of, Telephone Number, Program Name, Address, Program License Number, City, State, ZIP, SOS, and Page of, prior to submitting. Neglecting to accomplish that can produce an unfinished and probably nonvalid form!

Step 3: Prior to moving on, make certain that blank fields are filled out as intended. When you verify that it is correct, press “Done." Sign up with FormsPal right now and instantly access michigan form sos 258, prepared for downloading. Each change made is handily saved , making it possible to customize the form later as required. FormsPal provides protected form tools with no personal information record-keeping or any sort of sharing. Rest assured that your details are safe with us!