The South Dakota 55 form, a pivotal document overseen by the South Dakota Department of Labor and Regulation, serves as a crucial mechanism in the administration of unemployment insurance within the state. This form is formally recognized as the Application for Exemption or Transfer of Liability and is integral for business entities navigating changes in ownership, dissolution, or cessation of operation within South Dakota. Its primary function includes enabling businesses to either apply for exemption from the obligations tied to filing unemployment insurance reports or to facilitate the transfer of liability in instances of business acquisition or structural change. The detailed sections within the form call for precise identification of the business, including current owner or corporate name, business operating name (also known as DBA - Doing Business As), and contact information. Further, it outlines conditions under which a business might seek exemption or necessitate a transfer of unemployment insurance liability, demanding explicit disclosure regarding cessation of operations, business sale, or retention of any business fragment post-transaction. Additionally, it emphasizes the agreement on the transferal of the employer’s experience rating account, an essential element that can significantly impact the new owner's unemployment insurance cost responsibility. With directives for completion by the existing business owner, partner, or authorized official, the South Dakota 55 form underscores the technical aspects of business transitions while underpinning the state's commitment to maintaining operational fidelity and accountability in the realm of unemployment insurance.
| Question | Answer |
|---|---|
| Form Name | South Dakota Form 55 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | form55 sd forms 55 |
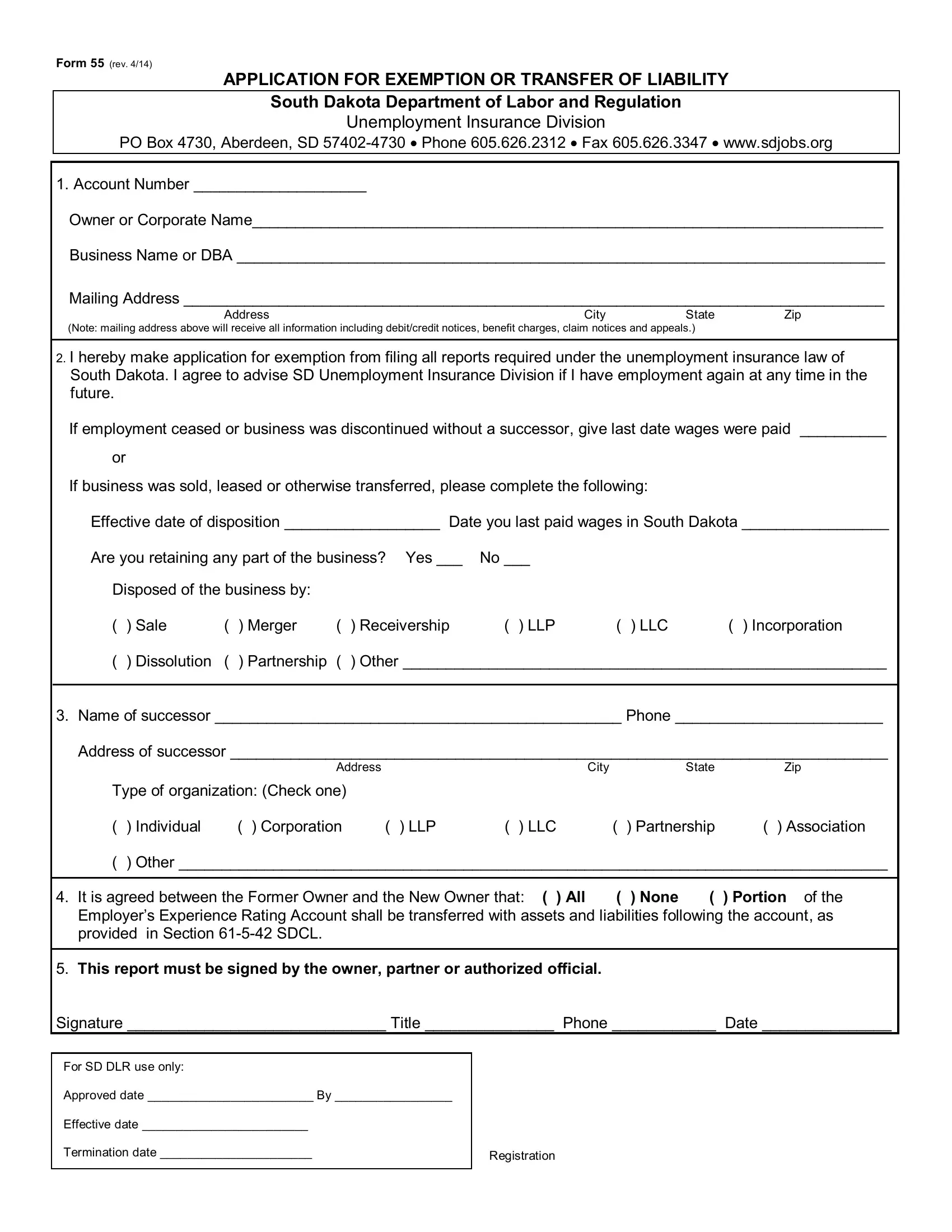
Form 55 (rev. 4/14)
APPLICATION FOR EXEMPTION OR TRANSFER OF LIABILITY
South Dakota Department of Labor and Regulation
Unemployment Insurance Division
PO Box 4730, Aberdeen, SD
1. Account Number ____________________
Owner or Corporate Name_________________________________________________________________________
Business Name or DBA ___________________________________________________________________________
Mailing Address _________________________________________________________________________________
Address |
City |
State |
Zip |
(Note: mailing address above will receive all information including debit/credit notices, benefit charges, claim notices and appeals.)
2.I hereby make application for exemption from filing all reports required under the unemployment insurance law of South Dakota. I agree to advise SD Unemployment Insurance Division if I have employment again at any time in the future.
If employment ceased or business was discontinued without a successor, give last date wages were paid __________
or
If business was sold, leased or otherwise transferred, please complete the following:
Effective date of disposition __________________ Date you last paid wages in South Dakota _________________
Are you retaining any part of the business? Yes ___ |
No ___ |
|
|
||
Disposed of the business by: |
|
|
|
|
|
( ) Sale |
( ) Merger |
( ) Receivership |
( ) LLP |
( ) LLC |
( ) Incorporation |
() Dissolution ( ) Partnership ( ) Other ________________________________________________________
3.Name of successor _______________________________________________ Phone ________________________
Address of successor ____________________________________________________________________________
|
Address |
|
|
City |
|
State |
Zip |
Type of organization: (Check one) |
|
|
|
|
|
|
|
( ) Individual |
( ) Corporation |
( ) LLP |
( ) LLC |
( |
) Partnership |
( ) Association |
|
( ) Other __________________________________________________________________________________ |
|||||||
|
|
|
|
|
|||
4. It is agreed between the Former Owner and the New Owner that: ( ) All |
( |
) None |
( |
) Portion of the |
|||
Employer’s Experience Rating Account shall be transferred with assets and liabilities following the account, as
provided in Section
5.This report must be signed by the owner, partner or authorized official.
Signature ______________________________ Title _______________ Phone ____________ Date _______________
For SD DLR use only:
Approved date ________________________ By _________________
Effective date ________________________
Termination date ______________________
Registration