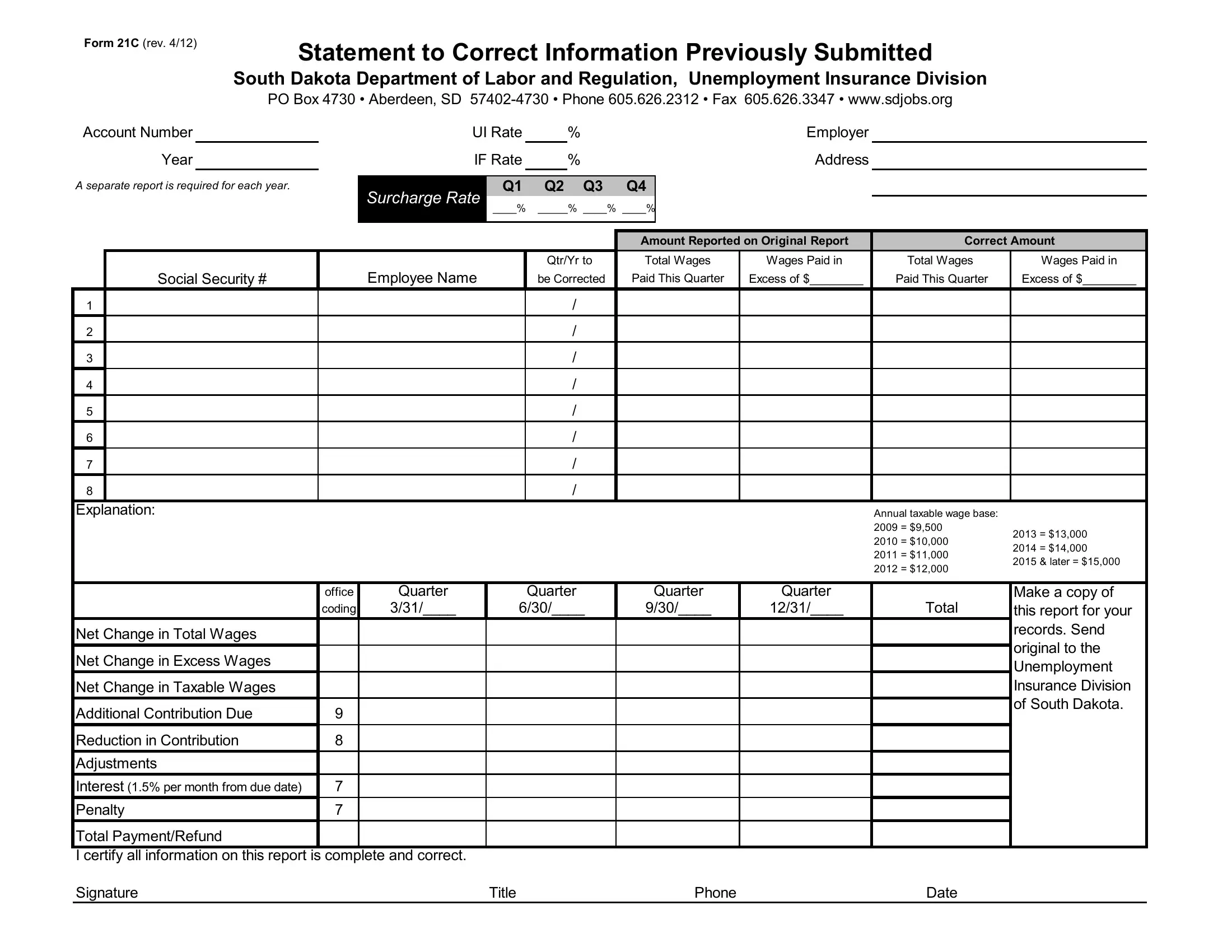
Efficient and accurate reporting is paramount for businesses, especially when it comes to matters of unemployment insurance. The South Dakota Form 21C serves as a crucial tool for employers within the state who need to correct previously submitted information regarding unemployment insurance. Revised in April 2012, this form is provided by the South Dakota Department of Labor and Regulation, Unemployment Insurance Division. It facilitates the amendments of key employer details such as account numbers, unemployment insurance rates, and the specifics of wages paid across different quarters. Employers are required to meticulously report the original and the corrected amounts for total wages paid, total wages in excess of the state's taxable wage base, along with the identification of each employee affected by these amendments. The form underlines the necessity of corrections for each quarter and year, reinforcing the state's commitment to maintaining accurate employment records. Besides offering a straightforward method to rectify previously submitted data, the form also plays a significant role in calculating any additional contributions due or refunds to be made, considering the adjustments in taxable wages, interest, and penalties. Its design underscores not just the importance of precision in unemployment insurance documentation but also aids in ensuring fairness and compliance in the employer's financial responsibilities towards it.
| Question | Answer |
|---|---|
| Form Name | South Dakota From 21C Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | form 21c drug license, form 21 drug license download, drug licence online verification, form 21c for drug licence |
Form 21C (rev. 4/12)
Statement to Correct Information Previously Submitted
South Dakota Department of Labor and Regulation, Unemployment Insurance Division
|
|
PO Box 4730 • Aberdeen, SD |
|
||||||||||
Account Number |
|
|
|
UI Rate |
|
% |
|
|
Employer |
|
|
||
|
Year |
|
|
IF Rate |
% |
|
|
Address |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A separate report is required for each year. |
|
Surcharge Rate |
Q1 |
Q2 Q3 |
Q4 |
|
|
|
|
||||
|
|
|
|
____% |
_____% ____% ____% |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Amount Reported on Original Report |
Correct Amount |
|||
|
|
|
|
|
|
|
Qtr/Yr to |
Total Wages |
Wages Paid in |
Total Wages |
Wages Paid in |
||
|
Social Security # |
|
Employee Name |
be Corrected |
Paid This Quarter |
Excess of $________ |
Paid This Quarter |
Excess of $________ |
|||||
1 |
|
|
|
|
|
|
/ |
|
|
|
|
|
|
2 |
|
|
|
|
|
|
/ |
|
|
|
|
|
|
3 |
|
|
|
|
|
|
/ |
|
|
|
|
|
|
4 |
|
|
|
|
|
|
/ |
|
|
|
|
|
|
5 |
|
|
|
|
|
|
/ |
|
|
|
|
|
|
6 |
|
|
|
|
|
|
/ |
|
|
|
|
|
|
7 |
|
|
|
|
|
|
/ |
|
|
|
|
|
|
8 |
|
|
|
|
|
|
/ |
|
|
|
|
|
|
Explanation: |
|
|
|
|
|
|
|
|
|
Annual taxable wage base: |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
2009 = $9,500 |
2013 = $13,000 |
|
|
|
|
|
|
|
|
|
|
|
|
2010 = $10,000 |
|
|
|
|
|
|
|
|
|
|
|
|
|
2014 = $14,000 |
|
|
|
|
|
|
|
|
|
|
|
|
|
2011 = $11,000 |
|
|
|
|
|
|
|
|
|
|
|
|
|
2015 & later = $15,000 |
|
|
|
|
|
|
|
|
|
|
|
|
|
2012 = $12,000 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
office |
Quarter |
|
|
Quarter |
Quarter |
Quarter |
|
Make a copy of |
||
|
|
|
coding |
3/31/____ |
|
6/30/____ |
9/30/____ |
12/31/____ |
Total |
this report for your |
|||
Net Change in Total Wages |
|
|
|
|
|
|
|
|
|
|
records. Send |
||
|
|
|
|
|
|
|
|
|
|
original to the |
|||
Net Change in Excess Wages |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
Unemployment |
|||
Net Change in Taxable Wages |
|
|
|
|
|
|
|
|
|
|
Insurance Division |
||
Additional Contribution Due |
9 |
|
|
|
|
|
|
|
|
|
of South Dakota. |
||
|
|
|
|
|
|
|
|
|
|
||||
Reduction in Contribution |
8 |
|
|
|
|
|
|
|
|
|
|
||
Adjustments |
|
|
|
|
|
|
|
|
|
|
|
||
Interest (1.5% per month from due date) |
7 |
|
|
|
|
|
|
|
|
|
|
||
Penalty |
7 |
|
|
|
|
|
|
|
|
|
|
||
Total Payment/Refund |
|
|
|
|
|
|
|
|
|
|
|
||
I certify all information on this report is complete and correct. |
|
|
|
|
|
|
|
|
|
||||
Signature |
|
|
|
Title |
|
|
|
Phone |
|
Date |
|
||
Form 21Cc (rev. 4/12)
Statement to Correct Information Previously Submitted
South Dakota Department of Labor and Regulation, Unemployment Insurance Division
PO Box 4730 • Aberdeen, SD
|
Account Number |
|
|
|
Employer |
|
|
|
Year |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Amount Reported on Original Return |
Correct Amount |
||
|
|
|
Qtr/Yr to |
Total Wages |
Wages Paid in |
Total Wages |
Wages Paid in |
|
Social Security # |
Employee Name |
be Corrected |
Paid This Quarter |
Excess of $_________ |
Paid This Quarter |
Excess of $_________ |
1 |
|
|
/ |
|
|
|
|
2 |
|
|
/ |
|
|
|
|
3 |
|
|
/ |
|
|
|
|
4 |
|
|
/ |
|
|
|
|
5 |
|
|
/ |
|
|
|
|
6 |
|
|
/ |
|
|
|
|
7 |
|
|
/ |
|
|
|
|
8 |
|
|
/ |
|
|
|
|
9 |
|
|
/ |
|
|
|
|
10 |
|
|
/ |
|
|
|
|
11 |
|
|
/ |
|
|
|
|
12 |
|
|
/ |
|
|
|
|
13 |
|
|
/ |
|
|
|
|
14 |
|
|
/ |
|
|
|
|
15 |
|
|
/ |
|
|
|
|
16 |
|
|
/ |
|
|
|
|
17 |
|
|
/ |
|
|
|
|
18 |
|
|
/ |
|
|
|
|
19 |
|
|
/ |
|
|
|
|
|
|
|
|
|
|
|
|
20 |
|
|
/ |
|
|
|
|
21 |
|
|
/ |
|
|
|
|
22 |
|
|
/ |
|
|
|
|